Expansile, mixed RL/RO lesion associated with impacted tooth #18
Can you make the correct diagnosis?
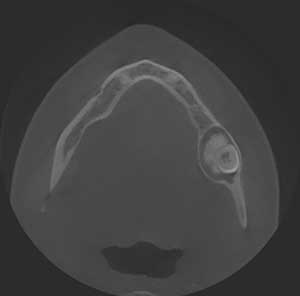
This is a 26-year-old female who had a panoramic radiograph taken in 2011 which showed an impacted tooth #18 associated with a mixed radiolucent-radiopaque lesion.
1. Complex Odontoma
2. Ameloblastic Fibro-Odontoma
3. Calcifying Odontogenic Cyst with Odontoma
4. CEOT (Pindborg tumor)
Sorry, you are incorrect!
A corticated, mixed RL/RO lesion with an obvious large opaque mass associated with an impacted/unerupted tooth should lead one to begin with odontoma as the most likely diagnosis. In this case, it would be a complex odontoma because it is in the form of a large opaque mass associated with an impacted molar tooth. Complex odontomas are usually associated with unerupted teeth in the posterior jaws, though they are more often associated with third molars than second molars. They can occur at any age but are more common in the first two decades of life. All of these characteristics are consistent with the age and clinical presentation of this patient. The slow growth over a six-year period, expansion, and relative lack of symptoms are also consistent with odontoma. Radiographically, the RL/RO and corticated lesion with a large RO mass is also typical of the radiographic changes of a complex odontoma. The histology, however, is not consistent with an odontoma.
Sorry, you are incorrect!
The clinical presentation of an impacted mandibular second molar tooth associated with a corticated RL/RO lesion should lead one to consider ameloblastic fibro-odontoma (AFO) on the differential diagnosis. This patient is older than the typical patient with this condition, since AFOs tend to occur in children around 10 years of age. They, too, are slow growing; therefore, the six-year duration of slow growth is also consistent with AFO, as is the expansion and lack of other clinical symptoms. The site in the mandible and the patient’s gender are also consistent with AFO since they have equal gender and jaw distribution. The radiographic findings of a well-circumscribed/corticated and expansile RL with RO mass is also consistent with AFO. The histology in this case, however, is not consistent with AFO.
Sorry, you are incorrect!
Calcifying odontogenic cysts (COC) generally occur in patients around 30 years of age with equal gender and jaw distribution. This clinical profile changes with COCs associated with odontomas (COC+O). Between 22% and 47% of COCs are associated with odontomas, including complex odontomas. In COC+O, the mean age is 16, and it is more common in females (F:M ratio 2:1) and slightly more common in the maxilla. The age and gender in this case are consistent with COC+O, but not the site. Nor is the association with impacted teeth common; fewer than 30% of COC+O cases are associated with impacted teeth. Radiographically, COC+Os are well-circumscribed RL with RO flecks or masses depending on whether it is COC alone or COC+O. The slow growth and expansion are also consistent with this condition. The histology, however, is not consistent with COC+O.
Congratulations, you are correct!
Pindborg tumor was first described in 1956 and constitutes less than 1% of odontogenic tumors. The age of this patient is young for this condition, since the typical age range is 30-50 years. The gender is consistent with this condition because Pindborg tumor has an equal gender distribution. The site is also consistent with this condition since close to 75% of Pindborg tumors occur in the posterior mandible. CEOT is expansile but otherwise asymptomatic, which is consistent with the behavior of this case. Furthermore, slightly more than 50% of CEOTs are associated with impacted teeth, as is the case with this patient. The slow growth in this case, however, is unusual for Pindborg tumor. Like ameloblastoma, Pindborg tumor is a benign but locally aggressive neoplasm. This lesion grew over a six-year period, but not aggressively. Radiographically, CEOT presents in several patterns ranging from a well-circumscribed unilocular radiolucency with radiopacity, as is the case in this patient, to a multilocular, “honeycomb” radiolucency with flecks of radiopaque material with so-called “driven snow” pattern (not shown in this case). The histology of this case is that of CEOT (Pindborg Tumor).