All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Large radiolucency: Left posterior maxilla and maxillary sinus
Contributed by: Dr. Craig Neal
Oral & Maxillofacial Surgery, Kirkland, WA
Case Summary and Diagnostic Information
This is a 6-year-old female who was referred to a pediatric dentist for evaluation of a recently noticed left cheek swelling (Figure 1).

This is a 6-year-old female who was referred to a pediatric dentist for evaluation of a recently noticed left cheek swelling. She was subsequently referred to an oral surgeon for the evaluation of a large vestibular swelling and cyst-like lesion involving the left maxilla. The CBCT revealed a large radiolucent lesion at the left posterior maxilla filling the left maxillary sinus (Figures 1-4). The lesion is pushing teeth apart and has focally extending into the lateral nasal wall. The swelling is not well demarcated.
Figure 1 This is a panoramic view of the CBCT imaging taken by the Oral Surgeon’s office at first clinical presentation. Note the large and diffuse radiolucency of the left posterior maxilla pushing teeth apart.

Figure 2 This is an axial view of the CBCT imaging taken at first clinical presentation demonstrating a large neoplasm expanding the buccally and filling the left maxillary sinus.
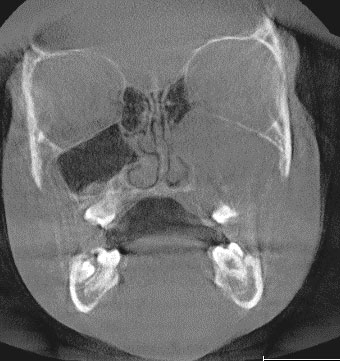
Figure 3 This is a coronal view of the CBCT imaging taken at first clinical presentation demonstrating a large neoplasm filling the left maxillary sinus and breaking through the bone in more than one area.

Figure 4 This is a sagittal view of the CBCT imaging taken at first clinical presentation demonstrating a large neoplasm displacing teeth and filling the left maxillary sinus.
The past medical history is not significant.
The swelling of the cheek was only recently noticed by the child’s parents. The duration of the left maxilla and maxillary sinus swelling is unknown. The lesion is displacing teeth and pushing them apart (Figures 1 & 4). Per CBCT, this lesion is also filling the maxillary sinus and expanding the bone (Figures 2-4). Clinically the maxillary vestibule shows fullness and loss of vestibular depth. It is asymptomatic and is somewhat firm to palpation and was not fluctuant. The swelling was not painful and there was no neural dysfunction.
Incisional biopsy was performed under IV sedation-the area was surgically exposed to show a relatively solid tumor grayish in color. The tumor peeled away from the overlying mucosa without difficulty. It had expanded through the lateral maxilla and filled the sinus. It was possible to begin exploring the edge of the lesion with a double ended curette by separating it from the mucosa and residual maxillary bone that surrounded it. Multiple fragments of tissue were biopsied and submitted for microscopic examination.
Histologic examination reveals multiple pieces of soft tissue composed of loose and myxoid connective tissue (Figure 5). It is made-up of stellate and small spindle-shaped fibroblasts suspended on delicate collagen fibers (Figures 6 & 7). In some areas, the myxoid connective tissue is hypocellular while in others it is slightly more cellular and has thicker collagen fibers. There is no evidence of an epithelial component or tumor-produced calcified material. There is evidence of host bone surrounded by the myxoid connective tissue. The immunohistochemistry stain is negative with S100 (not shown) which rules out myxoid peripheral nerve neoplasm.
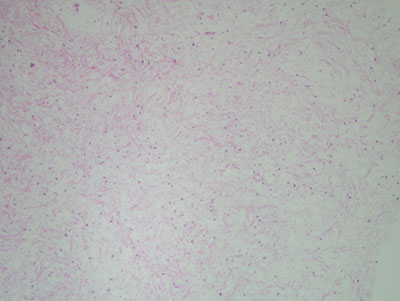
Figure 5 Low power (x40) H & E histology demonstrating myxoid and hypocellular fibrous connective tissue stroma made up of a small and stellate or spindle-shaped fibroblasts suspended on delicate collagen fibers and myxoid background.
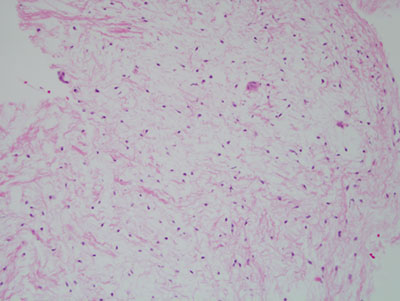
Figure 6 Higher power (x 100) H & E histology demonstrating the higher power of the histology described in Figure 4.
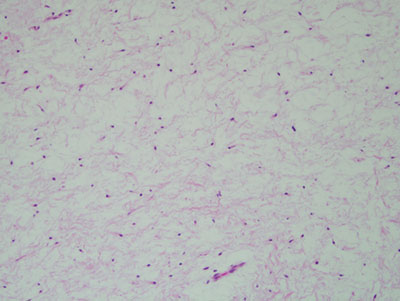
Figure 7 High power (x 200) H & E histology demonstrating the scant spindled shaped cells suspended on delicate collagen fibers and small blood vessels.
After you have finished reviewing the available diagnostic information