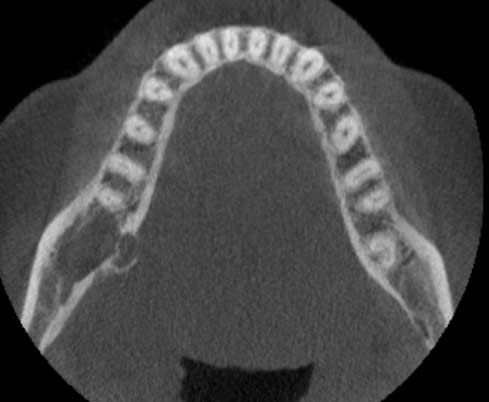
September 2018:Large radiolucency, right posterior mandible
Can you make the correct diagnosis?
This is a 38-year-old female with a history of a progressively enlarging swelling of the right posterior mandible over the last 2 to 3 years.
Sorry, you are incorrect!
The location in the posterior mandible, the slow growth, the expansion, the patient’s age and the radiolucency with a hint of multilocular appearance are all consistent with the clinical and radiographic presentation of solid ameloblastoma. The histology, however, is not consistent with ameloblastoma.
Ameloblastoma is one of the most common benign neoplasms of odontogenic origin. It accounts for 11% of all odontogenic neoplasms. It is a slow-growing, persistent, and locally aggressive neoplasm of odontogenic epithelial origin. Ameloblastomas usually expand the jaw bones and can perforate the jaw bone. It affects a wide age range with a mean of 33, with equal sex distribution. About 85% of ameloblastomas occur in the posterior mandible; most of these occur in the molar-ramus area, and some occur in the anterior mandible. About 15% occur in the maxilla. Radiographically, solid ameloblastomas typically present as multilocular and expansile radiolucencies.
Sorry, you are incorrect!
The neoplasm’s location, the obvious expansion, the patient’s age, the slow growth and the expansion with a hint of multilocular radiolucency are all consistent with odontogenic myxoma. The histology, however, is not consistent with odontogenic myxoma.
Odontogenic myxoma occurs in the jaw bones, usually in the tooth-bearing areas of the jaw. It is an uncommon, benign, and locally aggressive neoplasm. It has the potential for extensive bony destruction and perforation of bone into the surrounding structures. It is less common than ameloblastoma. Almost 75% of odontogenic myxomas occur in patients around 23-30 years of age with a slight female predilection (1:1.5 male-to-female ratio). It occurs almost equally in the maxilla and mandible with a slight predilection for the posterior mandible. A few cases are described in non-tooth-bearing areas including the ramus and condyle. Like ameloblastoma, odontogenic myxoma is slow-growing, persistent and destructive. Most cases are expansile and can displace and resorb teeth. In the maxilla, odontogenic myxomas usually invade the maxillary sinuses and, in rare cases, cross the midline to the opposing sinus. Radiographically, the majority present as expansile and multilocular, though some are unilocular with or without scalloped borders, and rare cases present with a diffuse and mottled appearance which can be mistaken for a malignant neoplasm.
Sorry, you are incorrect!
Intra-osseous hemangioma is exceedingly rare in the jaw bone, but the close proximity of the radiolucency to the inferior alveolar canal should bring this condition to the clinician’s mind.
The location, slow growth, radiolucent appearance, and the patient’s age and gender are all consistent with typical cases of intra-osseous hemangioma. The obvious expansion, however, is not typical of that condition, since they tend to expand only mildly. The histology in this case is not consistent with intra-osseous hemangioma.
Intra-osseous hemangiomas, especially those of the mandible and maxilla, are exceedingly rare. In other parts of the body, intraosseous hemangiomas comprise less than 1% of all hemangiomas and occur more commonly in the vertebrae and craniofacial bone, including the skull and the jaws, followed by long bones. They are slightly more common in females. In the jawbone, the mandible is affected three times as commonly as the maxilla. In the mandible, the body is the more common location, while the posterior mandible, the ramus, and the condyle are also sites that can be affected. Intra-osseous hemangiomas of the jaw tend to occur in the first three decades of life, while those of other bones tend to occur in older patients with peak incidence in the fifth decade. They are typically slow-growing and can be slightly expansile. Radiographically, intra-osseous hemangiomas commonly present as spider-web or multilocular radiolucencies but can present as unilocular radiolucencies or mixed radiolucent and radiopaque lesions.
Sorry, you are incorrect!
Intra-osseous schwannoma is rare in the jaw bones, but the close proximity of the expansile radiolucency to the inferior alveolar canal should bring to mind an intra-osseous peripheral nerve neoplasm.
The patient’s age, the lesion’s location, its slow growth, and its radiolucency are all consistent with that of an intra-osseous peripheral nerve neoplasm like schwannoma. The obvious expansion is also typical of that condition. However, this lesion was not painful, which suggests that an intra-osseous peripheral nerve neoplasm is a less likely diagnosis. The histology in this case is not consistent with intra-osseous schwannoma.
Intra-osseous schwannomas are rare. When they do occur, the posterior mandible is the most common location, typically in association with the inferior alveolar canal in the body and ramus area. This patient’s lesion is in the body of the mandible. The literature is clear that intra-osseous schwannomas of the jaws are by far more common in the mandible than in the maxilla. In one report of 44 cases, 39 of the specimens were from the mandible, especially the body and ramus of the mandible. They are usually associated with the inferior alveolar nerve and are often associated with pain, swelling and paresthesia. This patient did not have pain or paresthesia but there was obvious expansion. The average age for patients with this condition is 34, similar to that of the soft-tissue counterpart. Schwannomas, whether the soft tissue or intra-osseous type, are slow growing. Radiographically, intra-osseous schwannomas are well-circumscribed unilocular radiolucencies, but they can also be multilocular radiolucencies.
Congratulations, you are correct!
The site of occurrence and the patient’s age and gender are consistent with intra-osseous mucoepidermoid carcinoma (MEC). The radiographic findings are also consistent with this neoplasm. The histology in this case is consistent with low-grade mucoepidermoid carcinoma. It was determined via imaging that this lesion was of frankly primary intra-osseous origin—that is, it was not an extension of a primary MEC from the nearby submandibular glans or any other salivary gland tissue in the area. It was also determined that it was not a metastatic MEC.
Mucoepidermoid carcinoma is a malignant neoplasm of salivary gland origin that can present as a smooth-surfaced swelling or a non-healing ulcer on the soft tissue of the palate. While MEC accounts for 10% of all salivary gland neoplasms, the intra-osseous counterpart accounts for less than 2% of all MEC. It is therefore exceedingly rare for MEC to occur in the bone. The intra-osseous MEC tends to be more common in females and by far more common in the posterior mandible. Like its soft-tissue counterpart, intra-osseous MEC is described at all ages with greater prevalence around 4th and 5th decades of life.