All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
September 2018: Large radiolucency, right posterior mandible
Contributed by: Dr. Tyler McDonald
Central Washington Oral & Facial Surgery, Wenatchee, WA
Case Summary and Diagnostic Information
This is a 38-year-old female with a history of a progressively enlarging swelling of the right posterior mandible over the last 2 to 3 years.
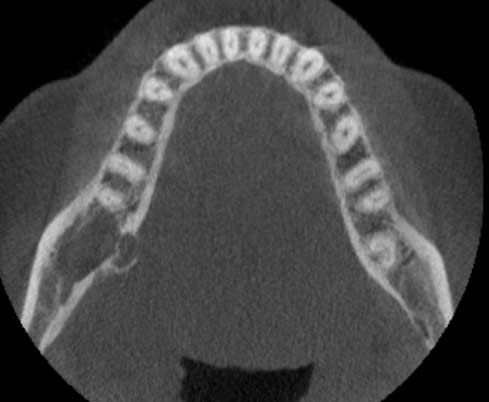
This is a 38-year-old female with a history of a progressively enlarging swelling of the right posterior mandible over the last 2 to 3 years. She presented to her dentist with the chief complaint of a swelling that started to push on her throat. She had no pain or any other systemic symptoms. A panoramic radiograph revealed a large radiolucency in the posterior mandible confirmed by a CBCT scan taken by the oral surgeon (Figures 1 & 2).
Figure 1 The CBCT axial view taken by the oral surgeon at first clinical presentation. Note the two compartment radiolucency expanding in the right posterior mandible expanding more lingually. It is thinning to focally perforating the lingual cortical bone. The radiolucency, however, seems to be well defined.

Figure 2The CBCT sagittal view taken by the oral surgeon at first clinical presentation. Note the well-defined radiolucency in the right posterior mandible apical to teeth #s 30 & 31.
The patient’s past medical history is significant for hypothyroidism, anxiety and chronic low back pain. Her medications include Duloxetine, Gabapentin, Levothryoxine and methocarbamol.
The patient’s chief medical complaint was of a swelling that started to push on her throat. This swelling was present for 2-3 years and was slowly and progressively enlarging. Otherwise she did not complain of pain or any other systemic symptoms. A panoramic radiograph revealed a large radiolucency in the posterior mandible confirmed by a CBCT scan taken by the oral surgeon (Figures 1 & 2).
Under local anesthesia, an incisional biopsy was performed. After the incisional biopsy, the patient was referred for surgical excision of the lesion.
Histologic examination of the H & E section revealed multiple pieces of soft tissue made up of an infiltrative neoplasm. The neoplasm is made up of mucous-producing cells surrounded by epidermoid cells arranged in a duct-like structure with cystic dilatation of some of the ducts (Figures 3 & 4). The mucous-producing cells comprise a significant portion of the neoplastic cells, while the epidermoid cells constitute a smaller portion and are mostly at the periphery of the cystic and duct-like structures lining the mucous producing cells (Figure 5). The neoplastic cells are suspended on mature connective tissue stroma.
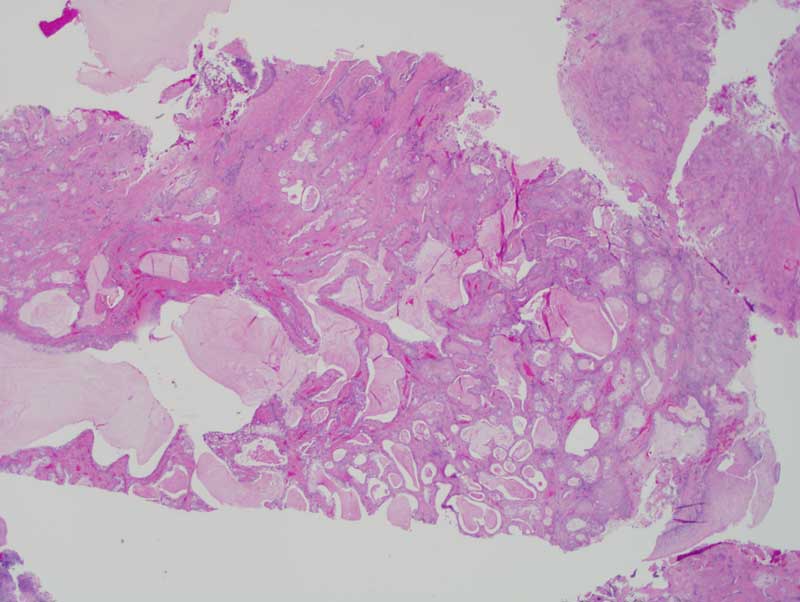
Figure 3 Low power (x40) H & E histology demonstrates infiltrative duct-like structures with cystic dilatation. These structures are lined by layers of mucous producing cells and epidermoid cells. The latter are at the periphery while the mucous producing cells are present intraluminally.
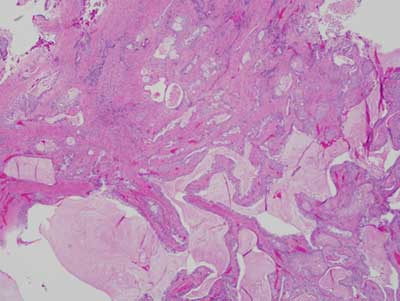
Figure 4 Higher power (x100) H & E histology demonstrates more with closer look at the duct-like and cystic structures with mucous producing cells and epidermoid cells at the periphery.
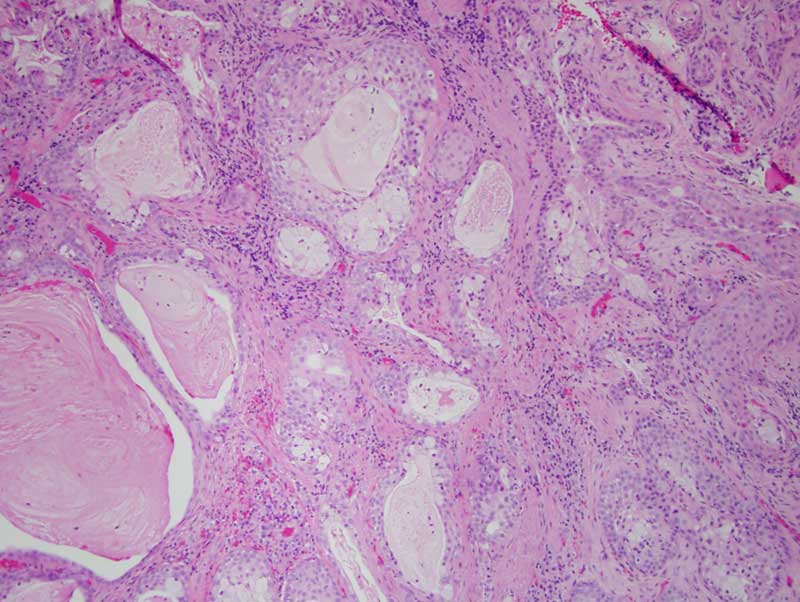
Figure 5 Higher power (x200) H & E histology offers a closer look at the duct-like structures with mucous producing cells and epidermoid cells at the periphery.
After you have finished reviewing the available diagnostic information