All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Large mixed radiolucent/radiopaque mass: Left maxilla & maxillary sinus
Contributed by:
Dr. Neal Futran, Andrew Nalley & Jeffrey Tuller
Otolaryngology & Oral Radiology, UW, Seattle, WA
Case Summary and Diagnostic Information
This is a 59-year-old female who noted a swelling in her left maxilla for a few months that she described as slow growing and painful.

This is a 59-year-old female who noted a swelling in her left maxilla for a few months that she described as slow growing and painful. Tooth mobility in the vicinity of the swelling was the main source of pain. Radiographic images revealed a large bony lesion, mixed radiolucent and radiopaque, in the left maxillary sinus and the entire left alveolar bone up to the midline involving the floor of the nose (Figures 1 & 2). Clinical examination revealed an expansile mass between teeth #s 9 and 15 involving the buccal, palatal and nasal components. The lesion did not involve the orbital floor or pterygoid-palate.
Figure 1 This is a panoramic view of the CBCT imaging taken at the clinical presentation. Note the large mixed radiolucent and radiopaque mass that fill the left maxillary sinus and involves the maxillary alveolar ridge. The superior maxillary sinus portion of the lesion is well-demarcated while the inferior alveolar ridge portion of the lesion is diffuse.
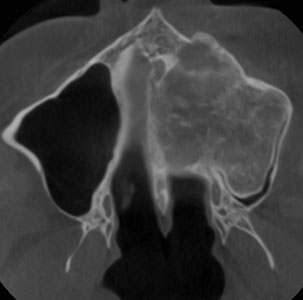
Figure 2 This is an axial view of the CBCT imaging taken at the clinical presentation demonstrating a large mixed radiolucent radiopaque lesion filling the entire left maxillary sinus.
In 2016, a lesion was surgically removed from this site. The patient’s past medical history is also significant for hypertension and GERD.
This condition has history dating back to 2016, when a slow-growing lesion in this area was excised. The patient did well until two months prior to presentation, at which point she developed pain and tooth mobility in this area. She presented with an expansile mass in the area between teeth #s 9 and 15 (Figures 1 & 2).
The patient was intubated and sedated for surgical removal of the lesion. A left maxillectomy was performed with an intraoral incision using Bovie cautery. Tooth #9 was extracted and soft tissue attachments dissected away. The mass was excised and hemostasis achieved using spatula tip Bovie cautery. The area was grafted using skin from the patient’s thigh, after which the area was packed with xeroform gauze. The premade obturator was then placed; it fit well and did not require placement of any screws. The patient recovered uneventfully.
Histologic examination reveals multiple pieces of soft tissue interspersed with new bone formation. The soft tissue is composed of cellular and vascular granulation tissue containing many giant cells (Figures 3 & 4). The granulation tissue is vascular and cellular. In focal areas, the granulation tissue is made-up of spindle-shaped cells arranged in bundles. These cells are mature and show no evidence of atypia. The giant cells are many and are of variable shapes and sizes (Figures 5 & 6). Also present are bony trabeculae; reflect mostly new bone formation.
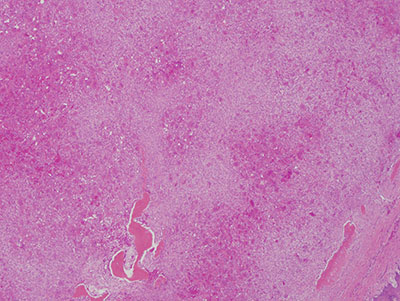
Figure 3 Low power (x40) H & E histology demonstrating cellular and vascular granulation tissue interspersed with many giant cells and small bony trabeculae.
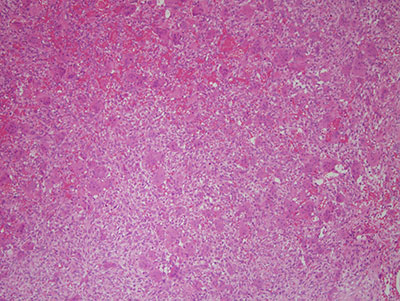
Figure 4 Higher power (x 100) H & E histology demonstrating a closer look at the cellular and vascular granulation tissue with many giant cells.
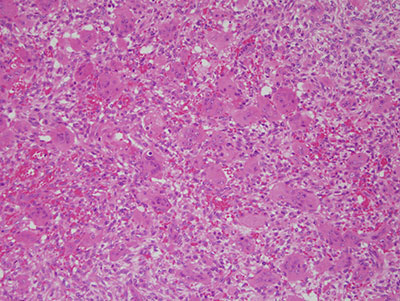
Figure 5 High power (x 100) H & E histology of more of the vascular and cellular granulation tissue many giant cells.
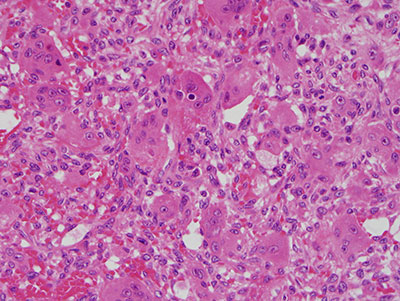
Figure 6 High power (x 200) H & E histology demonstrating the higher power of the many giant that are of variable shapes and sizes.
After you have finished reviewing the available diagnostic information