All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Large unilocular radiolucency associated with impacted tooth #17
Contributed by: Dr. Ross Beirne
Oral & Maxillofacial Surgery, UWSOD, WA
Case Summary and Diagnostic Information

This is a 16-year-old male who was referred by his general dentist to an oral surgeon for a left mandibular swelling.
This is a 16-year-old male who was referred by his general dentist to an oral surgeon for a left mandibular swelling. Panoramic radiograph reveals a very large and well-demarcated unilocular radiolucency associated with the crown of impacted tooth #17 (Figure 1). This radiolucency extends posteriorly close to the coronoid process and anteriorly past tooth #18. Bony perforation is noted in the ramus area. The expansion was intra-oral, mild, and more buccal. This swelling was first noted by the general dentist, not the patient; extra-orally, the face looked symmetrical.
Figure 1 This is a panoramic view taken at the first clinical presentation. The radiograph demonstrates a well-circumscribed and unilocular radiolucency around impacted tooth #17. There is thinning of the inferior border of the mandible and mild expansion.
The patient’s past medical history is unremarkable. There is no history of tobacco or alcohol use. The patient is not on any medications and has no known allergies.
This patient was referred to an oral surgeon for the evaluation of a swelling in the left posterior mandible noted in April 2017. All four third molar teeth were unerupted and tooth #17 was associated with a very large unilocular radiolucency with focal bony perforation. Tooth #18 did not show any mobility.
Histologic examination reveals a cystic structure lined by keratinized epithelium and supported by a cellular connective tissue wall. The lining epithelium is uniformly thin and corrugated and covered by a thin layer of parakeratin. The basal cell layer is palisaded (Figures 2 & 3). The connective tissue wall is cellular and infiltrated by lymphocytes and plasma cells.
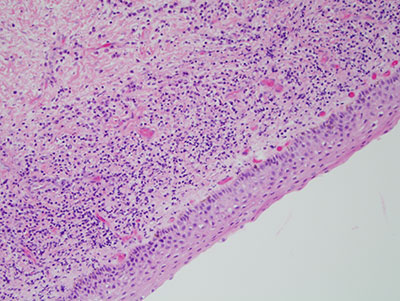
Figure 2 Lower power (x100) the H & E stained section shows a cystic structure lined by uniformly thin and keratinized epithelium. The basal cell layer is palisaded and connective tissue wall is mildly inflamed.
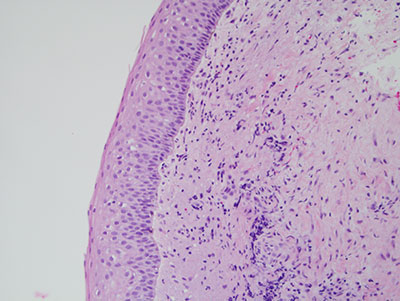
Figure 3 Higher power (x200) the H & E stained section shows a cystic structure lined by a thin layer of parakeratin. The epithelium is uniformly thin and the basal cell layer is palisaded.
Under deep IV sedation and general anesthesia, all four third molars were removed. In the area of tooth #17, the large cystic structure was removed and the area was thoroughly debrided and copiously irrigated. The patient demonstrated good healing and normal recovery. A follow up panoramic radiograph at two weeks showed a normal healing process (Figure 4).

Figure 4 This is a panoramic view taken two weeks after the surgical removal of the larger unilocular radiolucency and all four third molar teeth.
After you have finished reviewing the available diagnostic information