All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Large radiopaque expansile lesion; left posterior mandible
Contributed by: Dr. Calley Christie
Federal Way Oral & Maxillofacial Surgery, WA
Case Summary and Diagnostic Information
This is a 61-year-old female who presented with a chief complaint of a swelling in the left posterior mandible involving teeth # 18-20 extending buccally and lingually with radiographic findings of mixed radiolucent/radiopaque (RL/RO) lesion with “sunray” appearance.
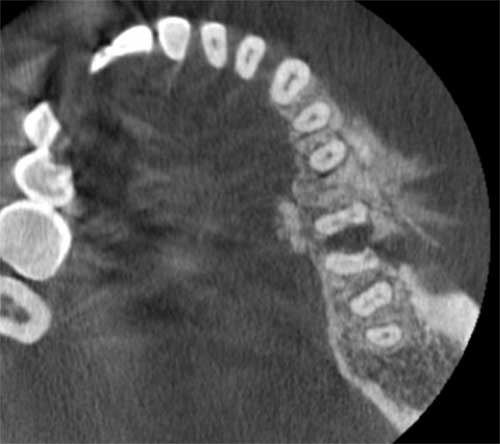
This is a 61-year-old female who presented with a chief complaint of a swelling in the left posterior mandible involving teeth # 18-20 extending buccally and lingually with radiographic findings of mixed radiolucent/radiopaque (RL/RO) lesion with “sunray” appearance (Figure 1). This lesion is reported to be of one year duration and was painless. No numbness was reported but it was displacing teeth #s 18 and 19 apart. The lesion was expansile and was described to be 3 X 3 cm in size.
Figure 1 This is an axial view of CBCT image demonstrating diffuse radiopaque lesion of the alveolar bone in area of teeth #s 18-20 with sunray appearance of bone protruding out of the alveolar bone vertically.
The patient’s past medical history is significant for tonsillectomy, breast reduction and hernia repair.
The patient presented with progressively growing gingival swelling of the left posterior mandible. The lesion continued to grow for about a year and the radiographic findings were those of a diffuse RL/RO lesion (Figure 1). Cone beam CT scan demonstrated an expansile mass centered on tooth #19 (Figure 2). Tooth #19 had a large decay.
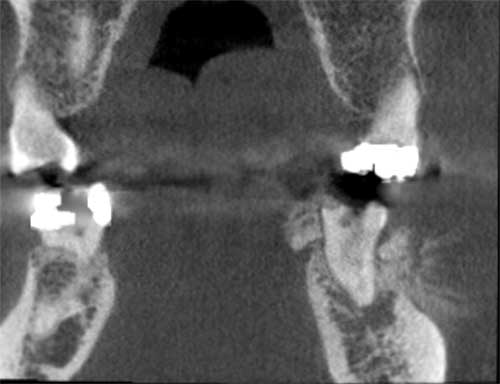
Figure 2 This is a coronal view of CBCT image demonstrating predominantly radiopaque lesion associated with tooth #19 in this view protruding mostly buccally but slightly lingual as well. The buccal bony projections have a sunray appearance.
Under local anesthesia, an incisional biopsy was performed and the results lead to the patient being referred for further evaluation.
The incisional biopsy revealed lobules of neoplastic cartilage that blend in with tumor bone (Figures 3-5) all surrounded by high-grade neoplastic soft tissue made up of spindle-shaped and stellate cells with hyperchromatic and angular nuclei exhibiting pleomorphism and significant number of mitotic cells (Figure 6).
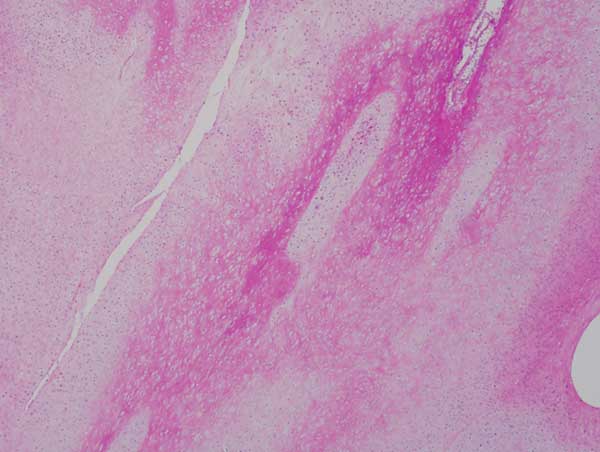
Figure 3 Low power (x40) H & E histology illustrates lobules of hard and soft tissue with neoplastic bone surrounding cartilage lobules partially surrounded by neoplastic spindle cells arranged in layers.
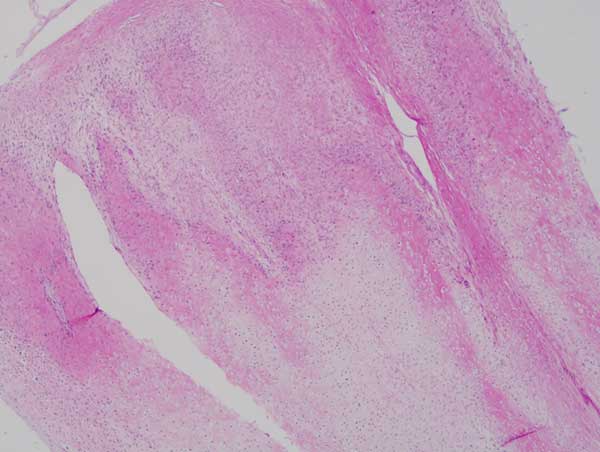
Figure 4 Higher power (x100) H & E histology with a closer look at the lobules of tumor bone and cartilage layered by neoplastic spindle shaped and angulated neoplastic cells.
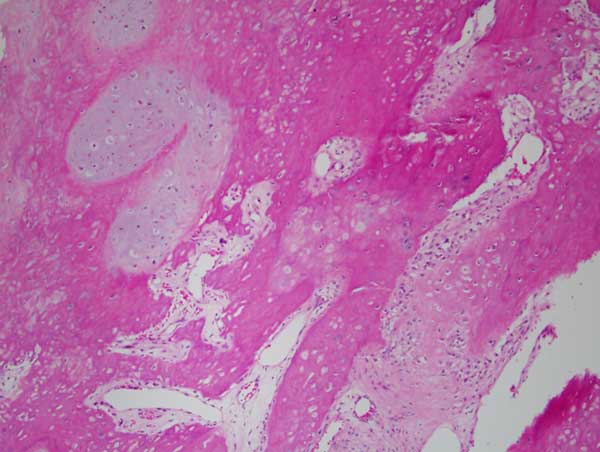
Figure 5 Higher power (x200) H & E histology with a closer look at tumor bone surrounding lobules of cartilage focally layered by neoplastic cells.
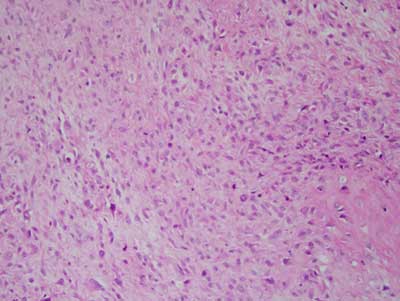
Figure 6 Higher power (x200) H & E histology with a closer look at the soft tissue component of this neoplasm made up of stellate and spindle-shaped cells with hyperchromatic and angulated nuclei and increased mitotic activity.
After you have finished reviewing the available diagnostic information