Large radiopaque expansile lesion; left posterior mandible
Can you make the correct diagnosis?
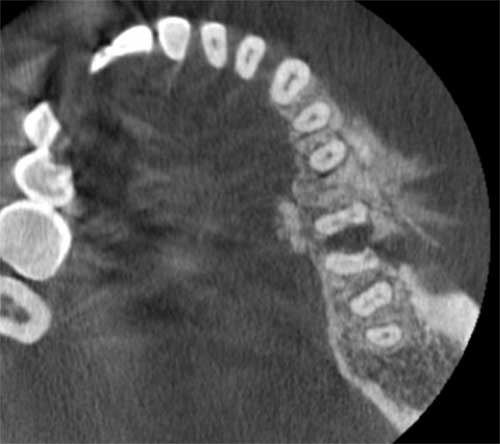
This is a 61-year-old female who presented with a chief complaint of a swelling in the left posterior mandible involving teeth # 18-20 extending buccally and lingually with radiographic findings of mixed radiolucent/radiopaque (RL/RO) lesion with “sunray” appearance
Sorry, you are incorrect!
The site, age and gender of this patient argue against a diagnosis of BPOP but some of the radiographic findings of a lesion arising from the surface bone with a broad base raised that question. The histology was not consistent with BPOP.
Bizarre parosteal osteochondromatous proliferation (BPOP); also known as Nora’s lesion is a benign and exceedingly rare lesion of bony origin that usually emerges from the surface of the cortical bone and is usually broad based. It is by far more common in small bone of hands but also affects the small bones of feet. Although described, it is exceptionally rare in the jaw bones. It is more common in males around the third and fourth decade of life. It is typically slow-growing and painless but can, on rare occasion, be painful. Radiographically, BPOP is a well-demarcated radiopaque mass with broad base connected to the surface of the cortical bone. Nora’s lesion is at times mistaken for parosteal osteosarcoma.
Congratulations, you are correct!
The site, radiographic and the clinical findings are consistent with osteosarcoma but not the age and gender. This patient is older than the mean of 33 years for jaw osteosarcomas. The histology is that of osteosarcoma-high grade.
Osteosarcoma is the most common, non-hematopoietic, primary malignancy of bone. It is a malignancy of mesenchymal cells that have the ability to produce osteoid or immature bone. Osteosarcoma of the jaw represents 6-9% of all osteosarcomas. Paget’s disease and prior radiation therapy are associated with an increased risk of developing osteosarcoma. The mean age for patients with jaw osteosarcomas is about 33 years, which is 10-15 years older than the mean age of osteosarcomas of the long bones. The posterior mandible is slightly more common.. Patients with osteosarcoma may experience pain, swelling, paresthesia and/or loosening of teeth. These tumors may vary greatly in radiographic presentation. Some lesions display an entirely radiolucent process, while others may demonstrate dense sclerosis in the affected area as is the case in this patient. However, the majority of osteosarcoma cases present as a mixed radiolucent and radiopaque lesions. Other radiographic findings include: symmetric widening of the periodontal ligament space (PDL), diffuse borders of the lesion, periosteal reaction, “spiked” roots or the classic “sunburst” or “sun ray” appearance caused by osteophytic bone deposition at the periphery. Osteosarcoma is a persistent malignancy. Osteosarcoma has an aggressive local growth potential and a propensity to spread systemically via hematogenous routes. The lung is the most frequent site of metastasis. Metastases from mandibular lesions are more frequent than from maxillary lesions. Today, therapy is typically multi-disciplinary, focusing on both local and systemic manifestations of osteosarcoma, thus incorporating surgery and chemotherapy. The use of this combined approach has resulted in a survival rate of 60-80%. In a 1997 study performed at the University of Washington, patients diagnosed with head and neck osteosarcoma had an overall 5-year survival rate of 72%.
Sorry, you are incorrect!
The gender, site and the bony expansion are all in support of central ossifying fibroma. The age is on the older age range and the radiographic findings lack the well demarcated/corticated border with a radiolucent rim that is typical of central ossifying fibroma. The histology is not that of COF.
Central ossifying fibroma is a benign neoplasm of bone origin. It presents as a well-demarcated to corticated radiolucent or mixed radiolucent/radiopaque mass with a peripheral radiolucent rim. Central ossifying fibroma is a slow-growing, expansile lesion with characteristic downward expansion of the inferior border of the mandible. It can also expand buccally and lingually. The associated teeth are vital. It is common in young adults around 35 years of age and is five times more likely to occur in females than males. It affects the posterior mandible in about 90% of cases. Curettage is the treatment of choice and recurrence is rare.
Sorry, you are incorrect!
There is one main reason why intra-osseous hemangioma is considered on the differential diagnosis of this case and that is related to the radiographic finding of “sunray appearance.” The differential diagnosis of the radiographic findings of “sunray appearance” includes osteosarcoma (more likely diagnosis) but IOH is also included because, on rare occasions, IOH can radiographically present with sunray appearance. Other, more minor factors that places IOH on the list of DDX is the site, being body of mandible and gender being slightly more common in females. The age is on the older age range for jaw IOH.
Intraosseous hemangiomas of the jaw (mandible and maxilla) are exceedingly rare but when they occur, they most commonly occur in the mandible (3:1 mandible over maxilla) and particularly in the body of the mandible. The age of jaw intraosseous hemangioma is more common in the first three decades of life. However, the literature related to other small bone IOH i.e. vertebrae and skull bone indicates that fifth decade is more common and that a wide age range of 2-85 is reported. These lesions tend to be slightly more common in females with a female to male ratio of 3:2. The radiographic findings of IOHs range from predominantly radiopaque to mostly radiolucent. The RL IOHs tend to present as unilocular, multilocular, or soap-bubble appearance. The IOH occasionally presents with a sunray appearance.