Unilocular radiolucency between teeth #s 28 & 29
Contributed by Dr. Peter E. Kim
Oral & Maxillofacial Surgery, Mount Vernon, WA
Case Summary and Diagnostic Information

This is a 55-year-old white male who was referred to Dr. Kim for the evaluation of a slowly growing swelling in the right posterior mandible.
This is a 55-year-old white male who was referred to Dr. Kim for the evaluation of a slowly growing swelling in the right posterior mandible (Figure 1). The panoramic radiograph shows a well-demarcated and partially corticated radiolucency between teeth #s 28 & 29. The patient noticed the swelling two weeks ago. The teeth were vital. There were no other symptoms—no pain or any other such symptoms.
Figure 1 This is a panoramic radiographic view taken at first presentation demonstrating a well-demarcated and partially corticated unilocular radiolucency between teeth #s 28 & 29. It is mildly displacing the two teeth.
The past medical history is significant for smoking 1ppd x 45 years. Past surgical history indicates mandibular advancement treatment.
The clinical examination revealed a nontender buccal swelling in the right posterior mandibular alveolar bone between teeth #s 28 and 29 (Figures 1). The panoramic radiograph demonstrates a well-defined and partially corticated unilocular radiolucency mildly pushing the teeth apart. Teeth #s 28 and 29 were vital. Wires at bilateral inferior border are consistent with the patient’s surgical history.
The surgical procedure was performed under local anesthesia. An incision was made from the anterior mandible in order to expose the buccal bone and the lesion was dissected and curetted. At his one-week follow up, the patient had no complaints, and no signs or symptoms of infection. Sutures were intact, and no drainage or numbness was noted.
The excisional biopsy revealed a cystic lesion lined by epithelium and supported by a fibrous connective tissue wall. The lining epithelium alternated between thin and thick, made up of one to three layers of cuboidal cells (Figure 2) alternating focally with proliferating epithelium forming small plaques (Figure 3). The connective tissue wall ranged from lose and cellular to fibrotic. Inflammatory cells are absent.
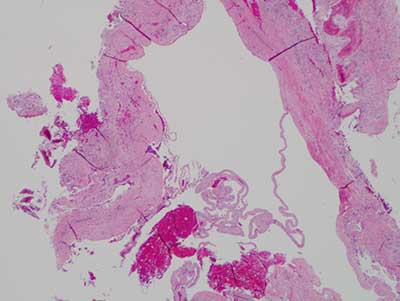
Figure 2 This is an H & E stained section at x 100 magnification demonstrating a cystic structure lined by epithelium supported by a fibrous connective tissue wall. The lining epithelium alternates between thin and thick. The thin epithelium is made up of cuboidal cells arranged in layers while the proliferative epithelium is arranged in plaques protruding into the lumen of this cyst.
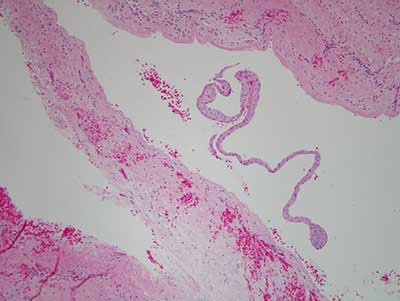
Figure 3 This is an H & E stained section at x 200 magnification demonstrating the proliferative epithelium forming plaques protruding into the lumen of this cyst.
After you have finished reviewing the available diagnostic information