All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Predominantly radiopaque lesion associated with unerupted tooth #3
Contributed by: Drs. Christopher “Kit” Steen and Yoo-Lee Yea
Bothell Oral & Maxillofacial Surgery, Bothell, WA
Case Summary and Diagnostic Information
This is a 7 1/2 year old male who presented with tooth #3 unerupted. There was no palpable expansion of the right posterior maxilla.

This is a 7 1/2 year old male who presented with tooth #3 unerupted. There was no palpable expansion of the right posterior maxilla. The panoramic and CBCT taken at presentation showed a 2.1 x 1.3 x 1.2 cm mixed but predominantly radiopaque lesion with foci of radiolucency at the right posterior maxilla associated with unerupted tooth #3 (Figure 1). This lesion extends into the right maxillary sinus (Figure 2).
Figure 1 This panoramic view was taken at first clinical presentation. It shows delayed eruption of tooth #3. This tooth is associated with a well-circumscribed RL/RO but predominantly RO mass. This image shows that the floor of the right maxillary sinus is lifted.

Figure 2 This coronal CBCT image was taken at first clinical presentation. It shows the large RO mass lifting the floor of the maxillary sinus and partially thinning the bone with the impression of extension into the sinus.
The patient’s past medical history is not contributory.
The panoramic radiograph shows a well-demarcated, large mostly radiopaque mass in the posterior maxilla associated with unerupted tooth #3 (Figure1). This lesion is of unknown duration and is not symptomatic.
The patient was treated under general endotracheal anesthesia. The lesion was approached via a right maxillary crestal/sulcular incision to broadly expose the right posterior maxilla. The lesion was encountered almost immediately, and was easily shelled out of its position at the floor of the maxillary sinus. A portion of the overlying gingivae was also excised, along the removal of the Cnidarian membrane. Tooth #3 was noted to be undisturbed in its crypt, and was not manipulated (Figure 3).

Figure 3 This panoramic view was taken post-surgery. Note that tooth #3 is left intact to allow it time to erupt.
Histologic examination reveals multiple pieces of decalcified hard and soft tissue composed of a benign neoplasm of mixed odontogenic origin (Figures 4-6). This neoplasm is made up of tooth-like structures cut tangentially (Figure 6). The hard tissue is surrounded by primitive connective tissue stroma containing nests, cords and small islands of odontogenic epithelium with palisaded and polarized columnar cells at the periphery (Figures 4).
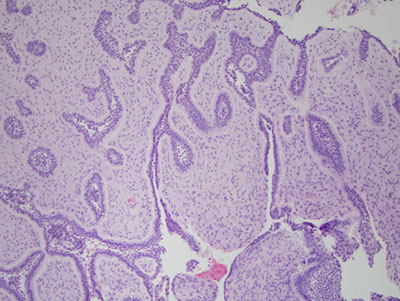
Figure 4 Low power (x40) H & E stained histology shows the soft tissue component of this neoplasm composed of primitive connective tissue and cords, islands and nests of odontogenic epithelial tissue. The periphery of these epithelial structures is lined by one layer of columnar, palisaded and polarized epithelial cells.
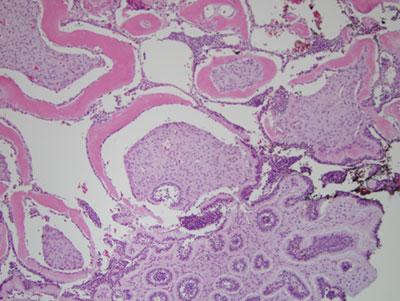
Figure 5 Higher power (x100) H & E stained histology shows a closer look at the neoplasm with mixed hard and soft tissue components. The soft tissue component is described in Figure 4 while the hard tissue component is made up of dentin.
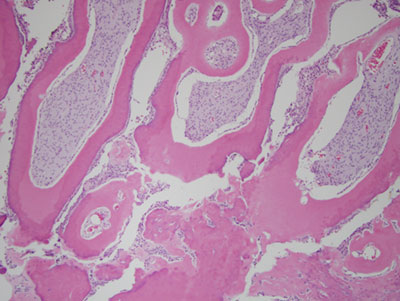
Figure 6 Higher power (x100) H & E stained histology shows a closer look at the hard tissue component of this neoplasm which is both normal dentin and dysplastic dentin and cementum.
After you have finished reviewing the available diagnostic information