Unilocular expansile radiolucency, right posterior mandible
Contributed by Dr. Gary Feldman
Oral & Maxillofacial Surgery, Seattle, WA
Case Summary and Diagnostic Information

This is a 64-year-old male who presented to a periodontal office for evaluation of a right mandibular edentulous bicuspid area for implant placement.
This is a 64-year-old male who presented to a periodontal office for evaluation of a right mandibular edentulous bicuspid area for implant placement. A well-demarcated expansile radiolucency was identified in the area and the patient was referred for a biopsy. Cone beam computed tomography (CBCT) was taken and shows a relatively well-demarcated expansile radiolucency in the right posterior mandible (Figure 1 & 2). The lesion was otherwise asymptomatic.
Figure 1 This is an axial cut of CBCT taken at presentation demonstrating buccally expansile unilocular radiolucency in the area of missing tooth #29.

Figure 2 This is a cross-sectional image of CBCT taken at presentation demonstrating a unilocular and expansile radiolucency in the right posterior mandible.
The patient’s past medical history is not contributory.
The CBCT images (Figure 1 & 2) demonstrated a well-demarcated and expansile radiolucency in the area of extracted tooth #29. This lesion is of unknown duration. It was discovered when the patient presented for evaluation of the area in preparation for implant placement.
Figure 1 This is an axial cut of CBCT taken at presentation demonstrating buccally expansile unilocular radiolucency in the area of missing tooth #29.
Figure 2 This is a cross-sectional image of CBCT taken at presentation demonstrating a unilocular and expansile radiolucency in the right posterior mandible.
Under local anesthesia, an incisional biopsy was performed and the specimen was send for histologic evaluation.
Histologic examination reveals multiple pieces of decalcified hard and soft tissue composed of fragments made up predominantly of granulation tissue with many giant cells (Figure 3). These are coalescing with fragments of a benign odontogenic neoplasm of mesenchymal origin containing remnants of odontogenic epithelium (Figure 4). The granulation tissue mass is loose and vascular with extravasated erythrocytes, small clusters of hemosiderin pigment and multinucleated giant cells. The neoplasm of odontogenic mesenchymal origin is made up of connective tissue stroma with strands and nests of epithelial cells of variable shapes and sizes. The epithelial component is highlighted with immunohistochemistry stain for pancytokeratin (Figure 5). The connective tissue stroma is made up of spindle shaped cells arranged in short bundles crisscrossing each other in some areas. Also present are fragments of lamellar and reparative bone with viable osteocytes and osteoblastic rimming.
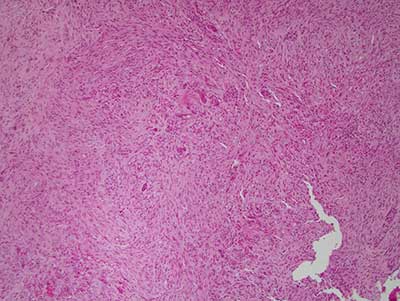
Figure 3 Low power (x100) H & E stained histology shows vascular and cellular granulation tissue with multinucleated giant cells.
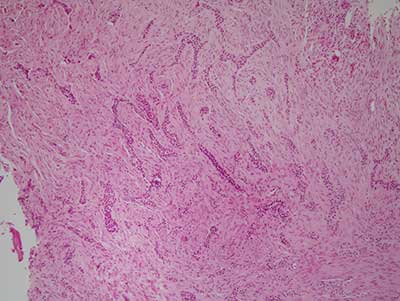
Figure 4 Low power (x100) H & E stained histology shows less vascular and more cellular mass of spindle-shaped cells interspersed with elongated cords and nests of odontogenic epithelial cells but no evidence of calcified material.
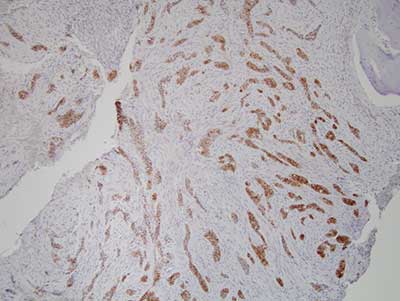
Figure 5 Higher power (x200) immunohistochemistry stain with pancytokeratin highlighting the epithelial cords and nests within the cellular connective tissue background.
After you have finished reviewing the available diagnostic information