All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Mass emerging from socket of extracted tooth-right posterior maxilla
Contributed by:
Dr. Daniel Brady
Oral & Maxillofacial Surgery, Everett-WA
Case Summary and Diagnostic Information
This is a 73-year-old female with dementia who was presented to a general dentist in October 2019 with a swelling and purulence drainage involving the right posterior maxillary teeth #s 2, 3, 4, and 5 which were extracted.

This is a 73-year-old female with dementia who was presented to a general dentist in October 2019 with a swelling and purulence drainage involving the right posterior maxillary teeth #s 2, 3, 4, and 5 which were extracted. A lot of purulent drainage was encountered coming from the extraction sites and the right nostril. The dentist sutured the extraction sites and placed the patient on antibiotics. The patient returned after one week for suture removal. The patient was recovering well and had no swelling or purulent drainage. At the end of November 2019, she presented with a mass emerging from the maxillary extraction socket (Figure 1) and the panoramic imaging showed the right maxillary sinus to be large and cloudy (Figure 2). She was referred for a consultation with an oral surgeon who biopsied the area.
Figure 1 This is a clinical photograph taken by the Oral Surgeon’s office at first clinical presentation. After the extraction all sockets healed but one. This is the non-healing socket with a large, exophytic and smooth surfaced pink nodule protruding from the right posterior maxilla into the oral cavity.
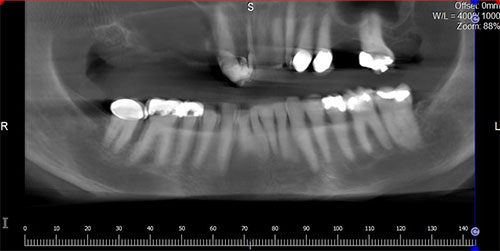
Figure 2 This is a panoramic view of the CBCT imaging taken by the oral Surgeon’s office at first clinical presentation demonstrating a large right maxillary sinus that is filled with this soft tissue appearing cloudy. Compare with the contralateral left maxillary sinus which is clear.
The past medical history is significant for dementia, hypertension and liver disease.
The 73-year-old female with dementia had multiple decayed and broken teeth in the right posterior maxilla that were extracted. At the time of extraction, multiple teeth were draining pus and the area was swollen. Patient was placed on antibiotics and the extraction sockets were sutured. The patient did well for the next few weeks but visited a dentist at end of November for an extraction site that had not healed. When the oral surgeon removed the soft tissue, he was surprised at the amount of tissue that emerged from the socket. At gross examination two soft tissue fragments were measured to 2.2 x 1.4 x 0.8 cm and 3.3 x 2.7 x 0.7 cm in aggregate which were submitted in three separate blocks for processing.
Incisional biopsy was performed under IV sedation
Histologic examination revealed multiple pieces of soft tissue composed of large papillary lesion (Figures 4-6) which occupied the bulk of the three blocks. The papillary projections were bulky and exophytic elongated and covered by multiple layers of oncocytes interspersed with mucous-producing cells. The epithelial cells of the papillary projections contained small clusters of neutrophils forming micro-abscesses.
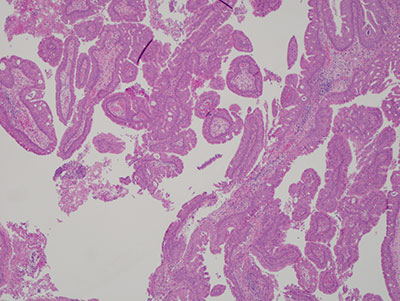
Figure 3 Low power (x40) H & E histology demonstrating many exophytic papillary projections lined by multiple layers of oncocytes. The papillary projections are supported by connective tissue core infiltrated by acute and chronic inflammatory cells.
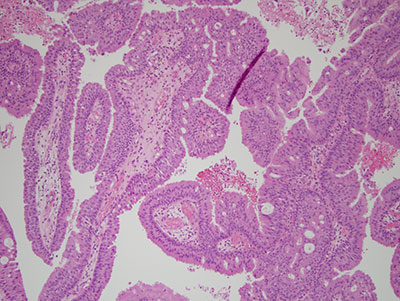
Figure 4 Higher power (x 100) H & E histology demonstrating the higher power of the papillary projections lined by oncocytes that are interspersed with mucous producing cells and contain small clusters of neutrophils forming micro-abscesses.
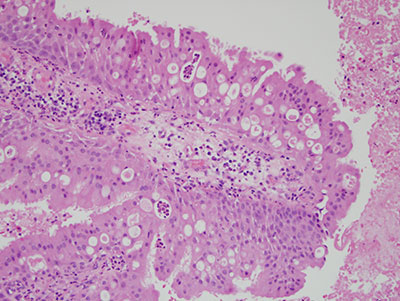
Figure 5 High power (x 200) H & E histology demonstrating the papillary projections with multiple layers of oncocytes, mucous cells and micro-abscesses.
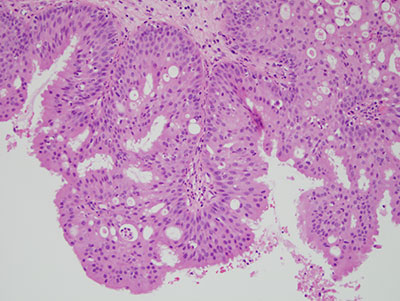
Figure 6 High power (x 200) of another area stained with H & E demonstrating histologic features similar to those in Figure 5.
After you have finished reviewing the available diagnostic information