All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Bilateral unilocular radiolucency associated with mandibular second molars
Contributed by: Dr. Calley Christie
Woodinville Oral & Maxillofacial Surgery, Woodinville, WA
Case Summary and Diagnostic Information
This is a 13-year-old white male who presented with mild swelling and tenderness in the left posterior mandible. The right posterior mandible was asymptomatic where no pain was reported or swelling noted.

This is a 13-year-old white male who presented with mild swelling and tenderness in the left posterior mandible. The right posterior mandible was asymptomatic where no pain was reported or swelling noted. However, a panoramic radiograph (Figure 1) revealed bilateral corticated unilocular radiolucencies associated with partially erupted teeth #s 18 and 31. Teeth are vital.
Figure 1 Panoramic view at first presentation demonstrating bilateral unilocular radiolucency with corticated border associated with partially erupted teeth #s 18 and 31.
The patient’s past medical history is negative for any systemic illness or surgery. The patient was placed on amoxicillin by the general dentist.
The panoramic radiograph demonstrates bilateral well-defined and corticated unilocular radiolucent lesions around partially erupted teeth #s 18 and 31. Although a well-demarcated radiolucency is identified on the right posterior mandible, the patient only complained of mild pain and swelling related to the left posterior mandible and not the right side. The buccal and lingual cortical bones of both sides were intact with no evidence of perforation.
Under IV sedation, full thickness mucoperiosteal flap was elevated from distal of #18 with releasing incision to mesial of tooth #20 to expose all the margins. A buccal plate window is made and the lesion is bluntly dissected and margins curetted and the area irrigated and closed with chromic suture. Similar procedure is performed on the right side where a mucoperiosteal flap is elevated from the distal of #31 to mesial of #30 exposing the buccal plate. The lesion is curette and the area is irrigated and closed with chromic suture.
Both specimens demonstrated similar histology. They will be described together. Multiple soft tissue fragments showed a large cystic structure lined by epithelium that was and supported by fibrous and granulation tissue wall (Figure 2). The lining epithelium was proliferative and non-keratinized stratified squamous in type and was spongiotic infiltrated by neutrophils (Figure 4). The fibrous and granulation tissue wall was infiltrated by many plasma cells, lymphocytes macrophages and neutrophils (Figures 3-4).
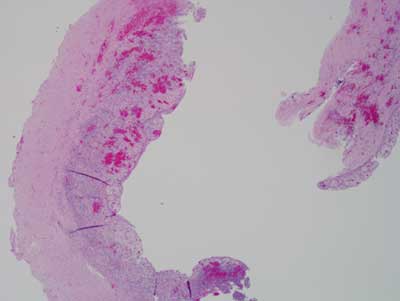
Figure 2 Low power (x40) H & E stained section shows a large cystic structure lined by non-keratinized epithelium and supported by fibrous and granulation tissue wall.
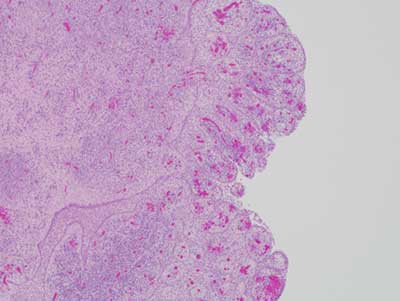
Figure 3 Higher power (x100) H & E stained section shows the cystic structure at a higher magnification. Both the lining epithelium and the connective tissue wall are heavily inflamed.
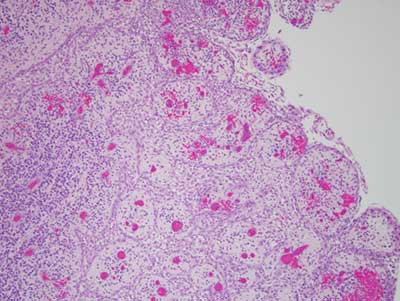
Figure 4 Higher power (x200) H & E stained section shows the lining epithelium at higher power. It is proliferative and spongiotic. It is infiltrated by neutrophils and lymphocytes.
After you have finished reviewing the available diagnostic information