Small unilocular radiolucent lesion mesial to tooth #21
Contributed by Dr. Jace Hansen & John Zhang
Idaho Perio Center & Labcorp Pathology, Idaho & WA
Case Summary and Diagnostic Information

This is a 68-year-old Caucasian female who presented to a periodontal office for evaluation of the area of extracted tooth #22 in preparation for the placement of a dental implant.
This is a 68-year-old Caucasian female who presented to a periodontal office for evaluation of the area of extracted tooth #22 in preparation for the placement of a dental implant. Cone beam computed tomography (CBCT) was taken to evaluate the alveolar bone thickness for the implant. The CBCT scan revealed a small, well demarcated radiolucent lesion on the mesial aspect of tooth #21 (Figures 1 & 2). The lesion was asymptomatic.
Figure 1 A panoramic CBCT view taken at presentation demonstrates a small, well-demarcated unilocular radiolucency mesial to tooth #21.

Figure 2 A three-dimensional CBCT view taken at presentation demonstrates a small, well-demarcated unilocular radiolucency mesial to tooth #21.
The patient’s past medical history is significant for seasonal allergies and high blood pressure.
This lesion was not symptomatic and was discovered while preparing to place an implant in the area.
Under local anesthesia, the area was treated with curettage and the specimen submitted for microscopic evaluation.
Histologic examination revealed two small pieces of soft tissue interspersed with calcified viable bone (Figure 3). The soft tissue component was predominantly composed of cellular and vascular granulation tissue with many multinucleated giant cells (Figures 3 & 4). The granulation tissue, however, was interspersed with slender strands of less vascular spindle-shaped fibroblasts surrounding nests of odontogenic epithelial cells (Figure 4). This portion of the specimen represented a benign neoplasm of mesenchymal odontogenic origin. The epithelial component is highlighted with an immunohistochemical stain for pancytokeratin (Figures 5 & 6).
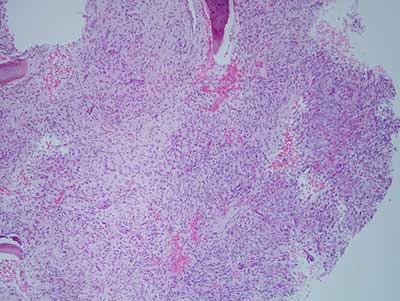
Figure 3 Low power (x100) H & E stained histology shows cellular and vascular granulation tissue with many multinucleated giant cells.
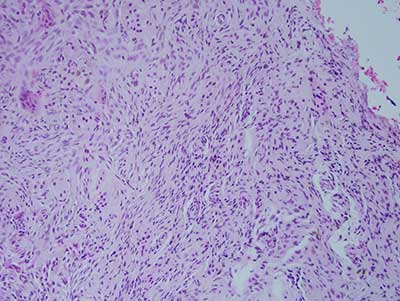
Figure 4 Low power (x100) H & E stained histology shows combined granulation tissue with giant cells interspersed with less vascular, spindle-shaped cells arranged in strands. Nests of epithelioid cells are also present.
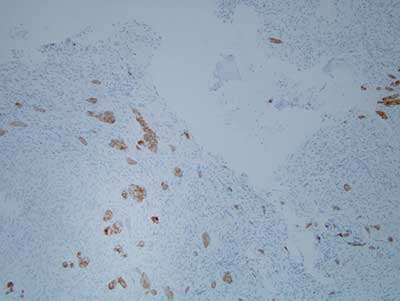
Figure 5 Low power (x100) immunohistochemical stain for pancytokeratin highlighting the epithelial cords and nests within the cellular connective tissue background.
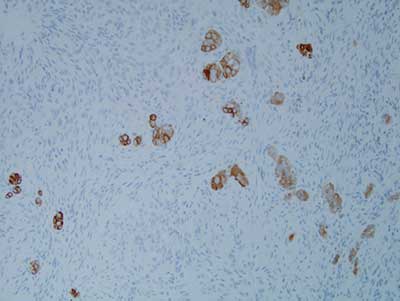
Figure 6 Higher power (x200) immunohistochemical stain for pancytokeratin highlighting the epithelial cords and nests.
After you have finished reviewing the available diagnostic information