Black Palate
Contributed by Drs. John Malan & Neal Futran
Montana Oral Surgery & UWMC Otolaryngology
Case Summary and Diagnostic Information

This is a 63-year-old male who presented to his dentist with the chief complaint of a palatal lesion that was of about one month’s duration.
This is a 63-year-old male who presented to his dentist with the chief complaint of a palatal lesion that was of about one month’s duration. The patient stated that about a month prior, he had started to notice roughness in his palate. He consulted with his dentist, who noted a diffuse discolored flat and nodular mass on the palate (Figure 1). The patient was referred for a biopsy. The patient’s health is otherwise stable with no symptoms related to swallowing or speech difficulty. There are no neck nodes or any other symptoms.
Figure 1 Clinical photograph of the lesion taken at the first visit. Note the diffuse, irregular black lesions on the palate; some are raised while others are flat. There lesion has irregular borders and the color lacks uniformity.
The patient’s past medical history is significant for rhinoplasty in 1980, malignant melanoma of the skin in 2004 successfully treated with surgery. The patient also had cataract surgery in 2009 and surgery on his right foot in 2008.
The patient felt a rough spot in his palate one month before the presentation (Figure 1). This did not cause him any difficulties with swallowing or speech, and there was no pain or numbness. Clinical examination revealed diffuse hyperpigmented lesions in the anterior and other parts of the hard palate. The lesion was irregular, was flat in some areas and slightly exophytic in others. The color was not uniform. The palate was the only site with these pigmented lesions; the rest of the oral cavity was clear of such lesions. There was no adenopathy and a PET scan was negative.
The lesion was biopsied under local anesthesia. The results of the incisional biopsy led to a referral to an ENT surgeon for further treatment. The patient underwent wide palatal resection with skin graft placement.
Histologic examination of the H & E section revealed surface epithelium with atypical melanocytes present within the surface and the deep lamina propria (Figure 2 & 3). The neoplastic melanocyte involved part of the superficial epithelium and mostly was deeply invasive into the connective tissue (Figures 2 & 3). The neoplastic cells were producing and releasing melanin (Figure 3). The immunohistochemistry stain was uniformly positive with Melan-A (Figure 4) and with antibody to S-100 protein (Figure 5).
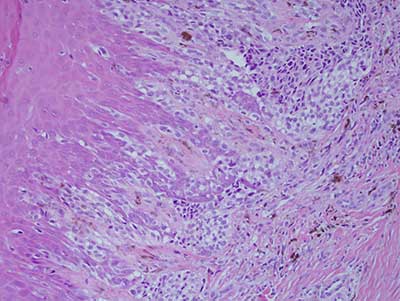
Figure 2 Low power (X100) histology shows H & E stained section with surface epithelium exhibiting atypical melanocytes extending upward with varying degrees nuclear pleomorphism and large nuclei with prominent nucleoli. The neoplastic cells are also invading the deep lamina propria in form of spindle-shaped cells producing and releasing melanin.
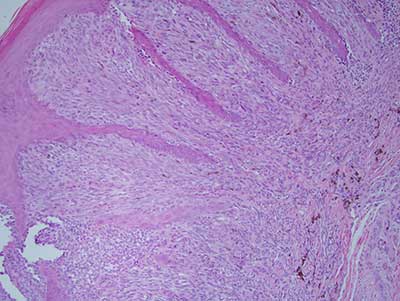
Figure 3 Higher power (X200) histology shows H & E stained section with surface epithelium exhibiting atypical melanocytes and underlying connective tissue with spindle-shaped neoplastic cells producing and releasing melanin.
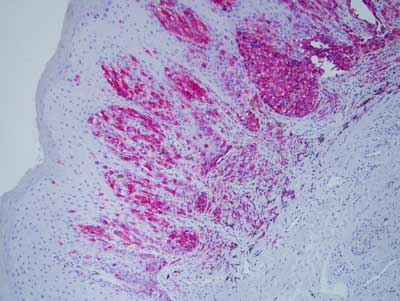
Figure 4 Low power (X100) Immunohistochemistry stain with Melan A antibody. Note the uniform positive neoplastic epithelial staining both in the surface epithelium and the underlying connective tissue.
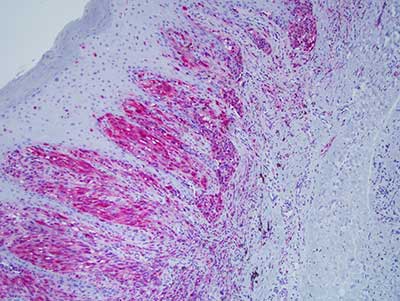
Figure 5 Low power (X100) Immunohistochemistry stain with S-100 protein. Note the uniform positive neoplastic epithelial staining both in the surface epithelium and the underlying connective tissue.
After you have finished reviewing the available diagnostic information