Ill-Defined Radiolucency; Left Posterior Mandible and Ramus
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by Dr. Robert Dixey
Oral & Maxillofacial Surgery, Bellevue, WA
Case Summary and Diagnostic Information
This is a 13-year-old white male who presented for an emergency exam of a large swelling in the left posterior mandible and ramus area.
Diagnostic Information Available
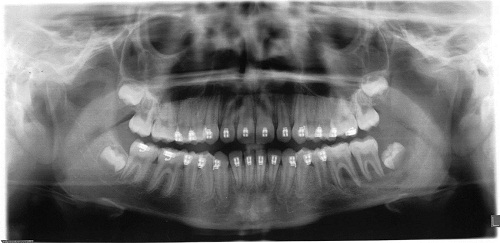
This is a 13-year-old white male who presented for an emergency exam of a large swelling in the left posterior mandible and ramus area. The clinical examination revealed a palpable mass that was slightly painful and was described to have intermittent bleeding episodes. Teeth #s 18 & 19 were slightly mobile. Patient states the problem started shortly before the braces were placed and the problem became worse after the braces were placed. Panoramic radiograph showed an ill-defined radiolucency involving the posterior mandible (teeth #s 17-19) extending superiorly into the ramus (Figure 1). The past medical history is negative.
Figure 1. Panoramic radiograph taken at first clinical presentation. Note the ill-defined radiolucency in the posterior mandible extending superiorly into the ramus. Also note the bone loss around teeth #s 18 & 19.
The past medical history is negative.
Clinical examination revealed a large mass of soft tissue in the left posterior mandible around teeth #s 17-19. Teeth #s 18 & 19 were slightly mobile. The mass was found to be associated with destructive bony lesion (Figure 1) involving teeth #s 17-19 and extending superiorly into the ramus.
Figure 1. Panoramic radiograph taken at first clinical presentation. Note the ill-defined radiolucency in the posterior mandible extending superiorly into the ramus. Also note the bone loss around teeth #s 18 & 19.
Treatment
Under intravenous anesthetic an incision was made over an intact buccal cortex. An incisional biopsy was performed and the tissue submitted for microscopic evaluation.
Incisional Biopsy
Histological examination revealed sheets and clusters of large cells with abundant cytoplasm and folded, grooved or bean-shaped nuclei intermixed with eosinophils and many multinucleated giant cells (Figures 2-4). The immunohistochemistry stain showed strong membrane expression with CD1a antibody (Figure 5). Mitotic figures were identified.
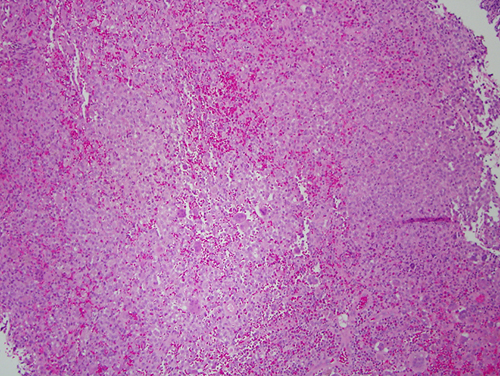
Figure 2. Low power (x40) H & E histology shows sheets of large round cells with abundant cytoplasm and many eosinophils.
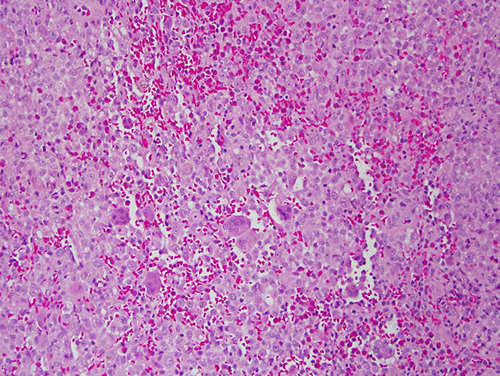
Figure 3. High power (x100) H & E histology shows sheets of large cells with abundant cytoplasm and folded nuclei intermixed with many eosinophils and multinucleated giant cells.
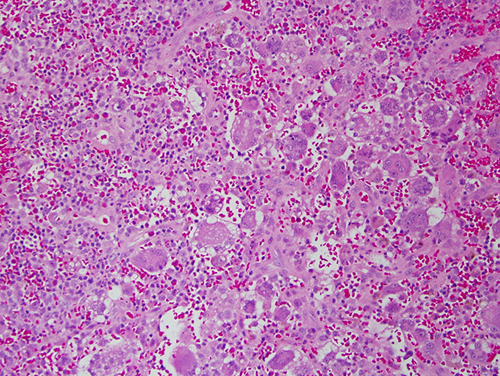
Figure 4. High power (x200) H & E histology shows many multinucleated giant cells surrounded by sheets of large cells with abundant cytoplasm and many eosinophils.
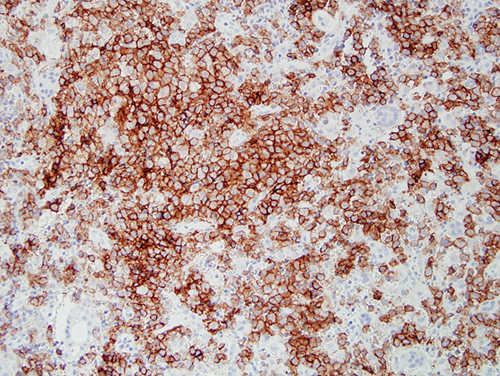
Figure 5. High power (x200) immunohistochemistry stain with CD1a antibody. Note the uniform and strong cell membrane positive stain.
After you have finished reviewing the available diagnostic information