All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Right mandible: mixed RL/RO Expansile Lesion
Contributed by:
Dr. Jeremiah Johnson
Central Washington Oral & Facial Surgery, Wenatchee, WA
Case Summary and Diagnostic Information
This is a 26-year-old male who was referred to an oral surgeon for the evaluation and treatment of his wisdom teeth and a large “cyst” involving tooth

This is a 26-year-old male who was referred to an oral surgeon for the evaluation and treatment of his wisdom teeth and a large “cyst” involving tooth #29 (Figure 1). The lesion was 15 x 16 x 20 mm in size. The patient reported that he could feel the swelling but that there was no pain in the area. He also confirmed that the wisdom teeth were not causing pain. The CBCT images demonstrate an expansile lesion (Figures 2 & 4). Figure 2 also shows flecks of radiopacity and a hint of multilocular morphology. Tooth #29 shows evidence of resorption and displacement.
Figure 1 This is a panoramic view demonstrating a large, well-demarcated radiolucency with a hint of multilocular appearance between teeth #s 27-30. Tooth #28 is missing for orthodontic reasons. Tooth #29 shows mild resorption.

Figure 2 This is a CBCT-coronal radiographic image of the posterior mandible demonstrating a buccally expansile radiolucency with flecks of radiopaque material. Note the hint of multilocular appearance.
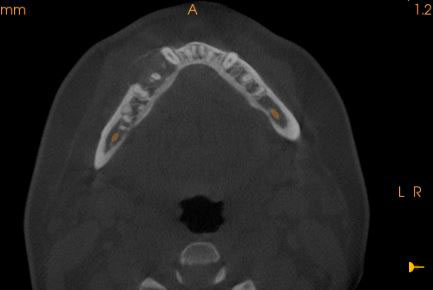
Figure 4 This is a CBCT-axial radiographic image of the posterior mandible demonstrating a buccally expansile and well-demarcated radiolucency with flecks of radiopacity.
The past medical history is unremarkable. The patient is otherwise healthy but reports daily cigarette smoking.
This patient was primarily referred for the evaluation of the wisdom teeth and the evaluation of an expansile lesion in the right mandible that was identified as a “cystic” structure. The expansile lesion is predominantly radiolucent (Figure 1), but has flecks of radiopaque material (Figures 2 & 3). Figures 2 & 4 show the significant buccal expansion.

Figure 3 This is a CBCT-reconstructed panoramic radiographic image of the posterior mandible. At this view, note the well-demarcated and predominantly radiolucent lesion with flecks of radiopacity
Under IV sedation and local anesthesia, a vestibular incision was made from the area of teeth numbers 27 to 30. The submucosal dissection exposed the lesion in the area. This area was entered with an 18-gauge needle, which yielded no aspiration. Superficial and deep specimens were removed and submitted for histologic evaluation. Teeth numbers 1, 16, 17 and 32 were surgically removed. There were no complications encountered during the surgery or post operatively.
Histologic examination revealed multiple pieces of decalcified hard and soft tissue composed of a benign fibro-osseous lesion (Figures 5-7). The specimens are made up of connective tissue stroma containing bony trabeculae at an early stage of development arranged in a trabecular manner (Figures 5 & 6). The bony trabeculae are lined by osteoblastic rimming (Figure 5). The connective tissue stroma is moderately cellular (Figure 6), composed of spindle-shaped cells suspended on delicate collagen fibers and small blood vessels. The stroma also contain multinucleated giant cells arranged in clusters (Figure 7).
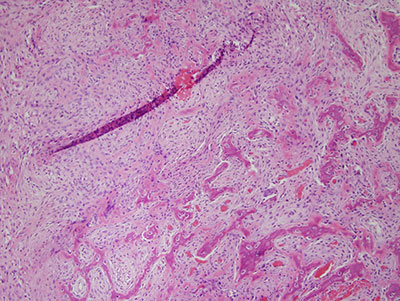
Figure 5 This is a low power (200X) micrograph of an H & E stained section, representing a decalcified fragment of benign fibro-osseous lesion with moderately cellular connective tissue stroma and early bony trabeculae formation with osteoblastic rimming.
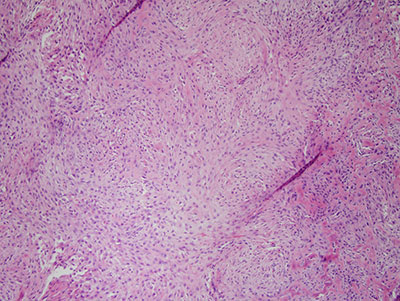
Figure 6 This is a higher power (200X) micrograph of an H & E stained section demonstrating the benign fibro-osseous lesion composed of cellular connective tissue stroma with spindle-shaped fibroblasts interlacing.
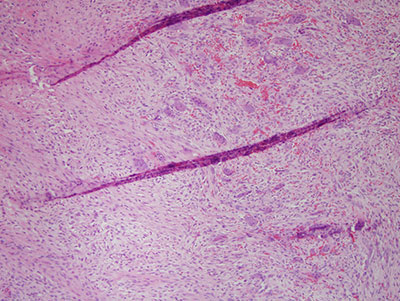
Figure 7 Higher power (x200) H & E stained histology demonstrating the bony trabeculae, with giant cells and cellular connective tissue stroma.
After you have finished reviewing the available diagnostic information