Return to Case of the Month Archives
Extensive superficial ulceration of the left ventral tongue
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Francis Collins
Oral Surgery, Wenatchee, WA
Case Summary and Diagnostic Information

This is an 87-year-old white female referred by her general dentist for the evaluation of a large, irregular, mostly superficial and ulcerated red and white lesion on the left lateral and ventral surfaces of tongue of unknown duration (Figure 1).
Diagnostic Information Available
This is an 87-year-old white female referred by her general dentist for the evaluation of a large, irregular, mostly superficial and ulcerated red and white lesion on the left lateral and ventral surfaces of tongue of unknown duration (Figure 1). The lesion was described to be associated with a badly broken molar tooth with sharp edges which her dentist had smoothed out three weeks previously with no resolution to the tongue lesion. She was subsequently referred for a biopsy. The patient complained of pain.
Figure 1 Photograph is taken at clinical presentation demonstrating a diffuse, mostly superficial red and white lesion on the left ventral and lateral tongue.
This patient’s past medical history is significant for right ear deafness and high blood pressure treated with hydrochlorothiazide. She has never used tobacco and rarely drinks alcohol.
This lesion is flat in most parts, irregular, red and white, and ulcerated. It involves almost half of the ventral surface of tongue and extends superficially to include the lateral border (Figure 1). In one area, mostly at the deep ventral surface, the lesion appears to be deep and ulcerated with rolled borders. The patient complained of pain and believed the lesion to be of traumatic origin from a sharp tooth.
Figure 1 Photograph is taken at clinical presentation demonstrating a diffuse, mostly superficial red and white lesion on the left ventral and lateral tongue.
Treatment
Under local anesthesia, a small biopsy was taken. The results of the incisional biopsy were such that the patient was referred to an ENT surgeon for definitive treatment.
Incisional Biopsy
Histological examination of the H & E section revealed surface epithelium exhibiting atypical epithelial changes and invading the underlying fibrous and skeletal muscle fibers. The atypical epithelial changes are manifested in large cells with prominent nuclei, cellular and nuclear disorganization and pleomorphism, loss of maturation, high mitotic activity, individual cell keratinization and keration pearls. The neoplastic epithelial cells invade the connective tissue and muscle fibers in form of small islands, nests and cords of cells. The connective tissue is also infiltrated by lymphocytes, plasma cells and neutrophils.
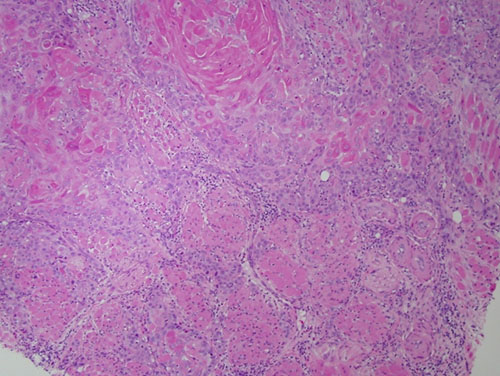
Figure 2 Low power (x100) the H & E histology reveals neoplastic epithelial islands invading the underlying connective tissue and skeletal muscle bundles.
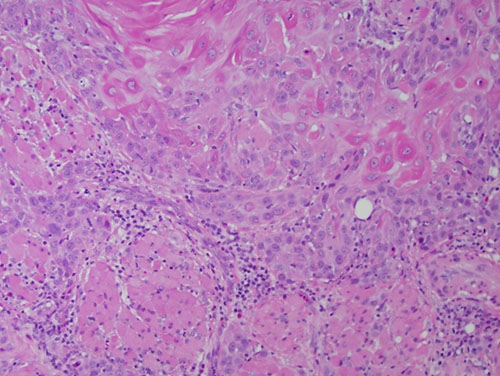
Figure 3 Low power (x200) the H & E histology of a slightly higher power shows the neoplastic epithelial cells invading the skeletal muscle bundles. The neoplastic cells show evidence of individual cell keratinization and a portion of a keratin pearl.
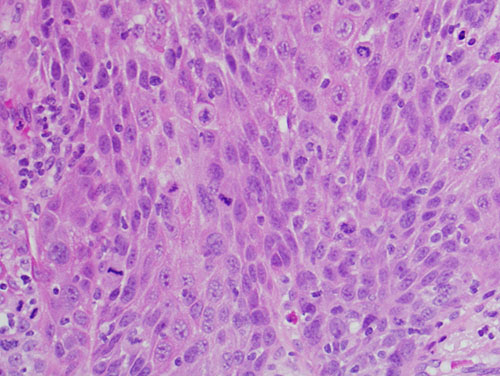
Figure 4 High power (x400) the H & E histology shows the neoplastic epithelial cells with high mitotic activity.
After you have finished reviewing the available diagnostic information