Nonhealing ulcer plus red & white lesion of left lateral tongue in nonsmoker
Contributed by Dr. Sukhdeep S Dhaliwal
Kitsap Oral & Maxillofacial Surgery, Silverdale, WA
Case Summary and Diagnostic Information

This is a 41-year-old white female who was referred to Dr. Dhaliwal for the evaluation of a red and white lesion with central ulceration on the left border lateral tongue.
This is a 41-year-old white female who was referred to Dr. Dhaliwal for the evaluation of a red and white lesion with central ulceration on the left border lateral tongue (Figure 1).
It measured 0.5 X 0.8 cm at its greatest dimensions. It was described to be painful and had been present for ~1 month.
Figure 1 This is an intra-oral photograph taken at first clinical presentation demonstrating a small 0.5 X 0.8 cm red and white lesion with small central ulceration of the left lateral tongue.
The past medical history is negative for tobacco use (never smoked) but is significant for diffuse Systemic Sclerosis (Scleroderma) since 2006.
The clinical examination revealed an irregular red and white lesion on the left lateral border tongue that was painful. It had been present for 1 month. No other lesions were noted on examination. There was no palpable cervical lymphadenopathy.
The procedure was performed under general anesthesia. An excisional biopsy was performed using cold steel. Bipolar electrocautery was used to obtain hemostasis. The surgical site was sutured and the area healed within a two-week period. The histology results indicated positive margins and wide local excision was needed for further treatment.
Histological evaluation of the incisional biopsy revealed a hemisected piece of soft tissue composed of surface epithelium exhibiting high-grade epithelial atypia, some invading the underlying connective tissue (Figures 2 & 3). The neoplastic cells invaded the underlying fibrous connective tissue and the skeletal muscle bundles in form of nets and islands. The neoplastic cells showed evidence of loss of maturation, nuclear hyperchromatism and alteration in the nuclear/cytoplasmic ration. Occasional cells with keratinization were present as well as few keratin pearls. The immunohistochemistry stain to p16, a surrogate antibody to oncogenic human papilloma virus (HPV), is negative (Figure 4).
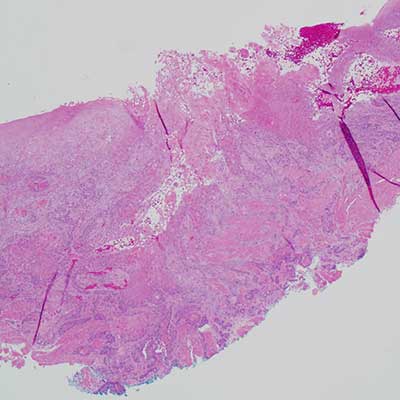
Figure 2 This is an H & E stained section at x 40 magnification showing a piece of mucosa covered by keratinized epithelium demonstrating superficial surface erosions/ulceration in the central portion of the specimen. The epithelium shows evidence of neoplastic changes, some invading the connective tissue and the underlying skeletal muscle bundles in form of islands and nests of cells. The epithelial cells show evidence of high-grade atypia in the form of nuclear hyperchromatism, loss of maturation, alteration in the nuclear/cytoplasmic changes and keratinization (both individual cell and keratin pearls).
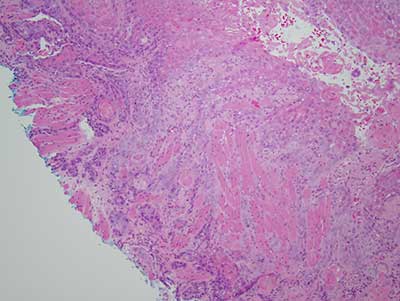
Figure 3 This is an H & E stained section at x 100 magnification with a closer look at the neoplastic cells invading the connective tissue and the underlying skeletal muscle bundles.
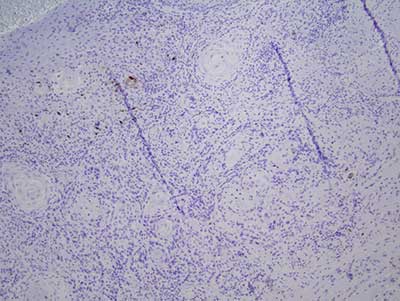
Figure 4 This is an immunohistochemistry stained section at x 100 magnification for p16 antibody, a surrogate antibody to oncogenic HPV; it is negative.
After you have finished reviewing the available diagnostic information