Single Large Swelling Right Posterior Maxillary Vestibule and Buccal Mucosa
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by Dr. David Cotant
Oral & Maxillofacial Surgery, Lakewood, WA
Case Summary and Diagnostic Information
This is a 47-year-old male who presented with a large, firm mass that was mobile within his cheek.
Diagnostic Information Available
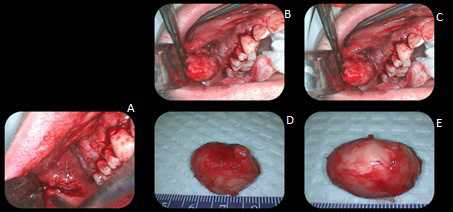
This is a 47-year-old male who presented with a large, firm mass that was mobile within his cheek. It had been progressively enlarging over a long period of time but the exact duration was unknown (Figure 1: A-C). The lesion was clinically described to be 2.5 x 2.0 x 2.0 at its greatest dimensions. It was otherwise not painful and had an intact oral mucosa. It was also described to be located lateral to the parotid gland papilla. The lesion was pink prior to surgery and yellow-tan when exposed. A panoramic radiograph showed no bony connection to the vestibular swelling.
Figure 1. This is a composite figure taken during the surgical removal of the specimen and represents the following: A-This photograph shows the swelling hanging down the vestibule covered by an intact oral mucosa. B & C-After a blunt incision through the vestibular mucosa, this photograph shows the swelling being exposed at different but close stages of the surgery. The swelling is round/oval and yellow-tan in color. It appears encapsulated. D & E: This photograph shows the gross morphology of the swelling. It is smooth-surfaced, yellow-tan and encapsulated.
The patient’s past medical history is significant for multiple cutaneous lipomas and multiple maxillary buccal exostoses.
The patient reported a slowly enlarging nodule in his right maxillary vestibule that had been present for an unknown period of time. The swelling was mobile and not painful and the overlying mucosa was intact.
Treatment
Under local anesthesia, an incision through the mucosa was performed where an encapsulated yellow-tan nodule was released (Figure 1: D & E).
Excisional Biopsy
Histologic examination reveals a large and multisected piece of soft tissue composed of an encapsulated neoplasm of salivary gland origin (Figure 2). It is partly made up of duct-like structures surrounded by one to two layers of cuboidal epithelial cells and focally filled with an eosinophilic coagulum (Figure 3). The ducts are of variable sizes and shapes, some dilated. The second component is myoepithelial cells which are arranged in a variety of patterns, including round cells with abundant cytoplasm and some arranged in a spindle-shaped manner (Figures 2-4). In most parts, the neoplastic cells are suspended on a chondromyxoid mesenchymal background (Figures 2-4).
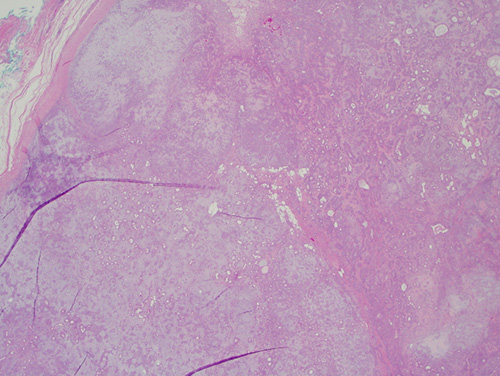
Figure 2. Low power (x20): the H & E histology reveals an encapsulated neoplasm composed of many ducts of variable shapes and sizes surrounded by other type of cells, all suspended on a lobular chondromyxoid mesenchymal background.
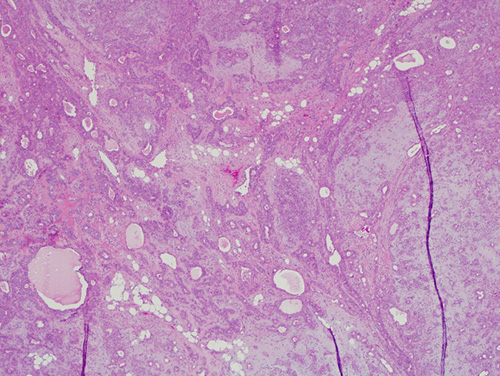
Figure 3. Low power (x100): the H & E histology reveals a neoplasm composed of many ducts surrounded by cuboidal epithelial cells and some filled with an eosinophilic coagulum. Also present are round cells with abundant cytoplasm and spindle-shaped cells all consistent with myoepithelial cells. All neoplastic cells are suspended on a chondromyxoid mesenchymal background.
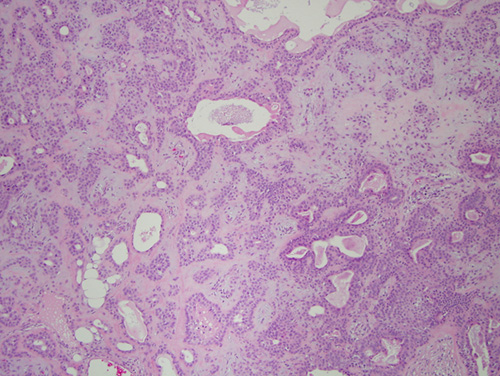
Figure 4. High power (x200): the H & E histology reveals a neoplasm with ducts lined by cuboidal epithelial cells and surrounded by myoepithelial cells.
After you have finished reviewing the available diagnostic information