Return to Case of the Month Archives
Severe Generalized Gingivitis/Periodontitis and Bleeding
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Robert C Zalme, COL, USAF; Dr. Carroll A Palmore, COL, USAF; Dr. Timothy J. Halligan, COL, USAF; Dr. Nathan G. Russell, CAPT, USAF; Dr. Steven J. Caldroney, CAPT, USAF;
Keesler Medical Center, Keesler Air Force Base, Mississippi
Case Summary and Diagnostic Information

This is a 39-year-old white female with a history of mental retardation. She presented in August 2003 to Hospital Dentistry for severe periodontitis, halitosis and loose teeth.
Diagnostic Information Available
This is a 39-year-old white female with a history of mental retardation. She presented in August 2003 to Hospital Dentistry for severe periodontitis, halitosis and loose teeth (Fig 1-3). In September 2003 she presented to Keesler Medical Center emergency room and was later admitted to the hospital for an unspecified protein-calorie malnutrition, anemia and hypokalemia (her potassium level was 2.5mmol/L; the normal level is 3.6-5.1 mmol/L). She also had severe periodontitis and calculus accumulation. Her diet consisted entirely of Kraft Mac and Cheese, peanut butter and soda. Her mother did not recall vegetables or fruits in her daughter’s diet.
Figure 1. Patient at presentation demonstrating, swollen, red gingiva and bleeding and ulcerated lips.

Figure 2. Patient at presentation demonstrating severe periodontitis and focal gingival bleeding.

Figure 3. Panoramic view at first presentation demonstrating severe periodontitis and calculus accumulation.
The patient’s past medical history is negative for allergies, alcohol or tobacco use, any continuous medication intake, hospitalization or malignancies. Her father died of Kaposi’s sarcoma.
The patient presented with severe periodontal disease (Fig 1-3), swollen, red and boggy gingiva, severe calculus, loose teeth, and gingival hemorrhage. The panoramic radiograph showed extensive bone loss and calculus accumulation. She also had extensive cutaneous bruising, especially on the extremities (Fig 4); petechiae; poor and delayed wound healing; lower extremity edema and a non-healing ulcer on the upper arm. She also complained of myalgia and limited range of motion in legs and ankles. The patient also had anemia.
Figure 3. Panoramic view at first presentation demonstrating severe periodontitis and calculus accumulation.

Figure 4. Patient at presentation demonstrating extensive cutaneous bleeding.
The histology showed evidence of exuberant granulation tissue with focal surface ulcerations, congested blood vessels, extravasated erythrocytes and acute and chronic inflammatory infiltrate consistent with chronic gingivitis (Figs. 7-8). The biopsy was performed by Dr. Zalme. The photographs were kindly provided by Dr. Zalme.
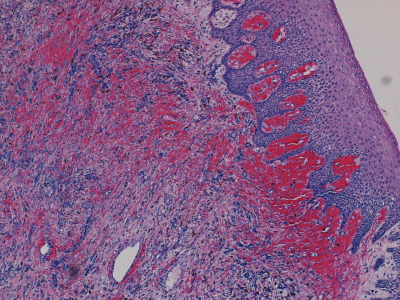
Figure 7. Low power (x200) histology shows dense vascular granulation tissue with clusters of extravasated erythrocytes in the superficial lamina propria.
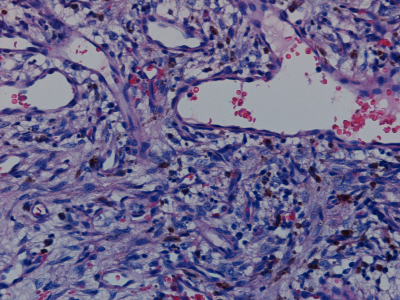
Figure 8. High power (x400) granulation tissue with many blood vessels, some dilated and clusters of brown pigment consistent with hemosiderin.
After you have finished reviewing the available diagnostic information