All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Expansile radiolucency, right posterior mandible
Contributed by: Dr. Todd Carter
Maui Oral & Maxillofacial Surgery-Hawaii
Case Summary and Diagnostic Information
This is a 72-year-old male who visited his dentist with a chief complaint of pain in the right posterior mandible associated with the only intact tooth remaining in his mouth.
This is a 72-year-old male who visited his dentist with a chief complaint of pain in the right posterior mandible associated with the only intact tooth remaining in his mouth. The tooth had significant mobility. The panoramic radiograph showed a single tooth with severe periodontitis involving the periapical area (Figure 1). Clinically, there was right facial swelling and a hard mass palpable at the right angle of the mandible. CBCT images displayed a large expansile radiolucency at the right posterior mandible with perforation of the cortices as well as mildly scalloped borders (Figure 2). The patient’s past medical history is significant for nephrolithiasis, hypertension, hypercholesteremia and type II diabetes.
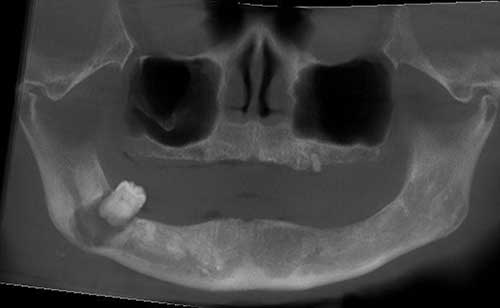
Figure 1 Panoramic radiograph taken at first clinical presentation demonstrating an almost completely edentulous upper and lower jaw except for tooth #32 and a retained root in the left maxilla. Tooth #32 shows severe periodontitis involving the apices.
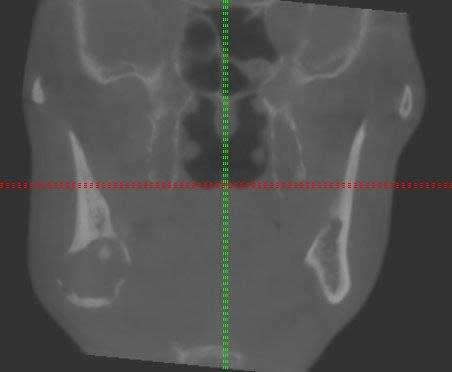
Figure 2 CBCT radiographic view demonstrating a unilocular, expansile radiolucency in the right posterior mandible with slightly scalloped borders perforating bone.
This patient’s past medical history is significant for nephrolithiasis, hypertension, hypercholesterolemia and type II diabetes. He is on Atorvastatin, Lisinopril and glipizide.
This 72-year-male presented to the general dentist complaining of pain associated with his only remaining tooth, #32. He also was seeking complete dentures. The dentist obtained a panoramic radiograph (Figure 1) and noted a large radiolucency as well as an acute purulent infection with a mobile tooth #32. The patient was started on clindamycin for the infection and referred to an oral surgeon for evaluation who noticed right-side facial swelling and a hard palpable mass in the right angle region. An intraoral exam revealed almost edentulous jaws with the exception of a mobile tooth #32 and a retained root in the left maxilla. The mobile tooth #32 was surrounded by erythematous soft tissue and released purulence from the sulcus. A CBCT was obtained; it showed a large and expansile radiolucency in the right angle of the mandible perforating the facial and labial cortices with mildly scalloped borders (Figure 2).
Under local anesthesia, tooth #32 was extracted, yielding purulent discharge and an empty appearing socket with thick walled soft tissues around the margins. Some of the soft tissue lining was curetted and submitted for histologic evaluation.
Histologic examination of the H & E section revealed multiple pieces of soft tissue composed of fibrous and cellular granulation tissue lined by epithelium (Figures 3-5). The epithelium was proliferative and stratified squamous in type, ranging from nonkeratinized (Figure 3) to keratinized (Figure 4). The epithelium was focally spongiotic and infiltrated by neutrophils (Figure 5). The fibrous and granulation tissue was intensely infiltrated by neutrophils, plasma cells, lymphocytes and some macrophages (Figures 3-5).
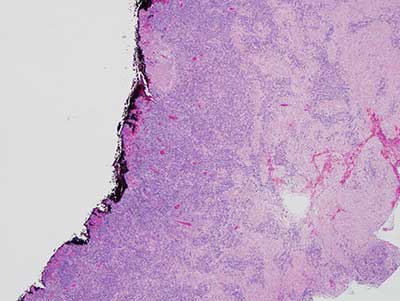
Figure 3 Low power (X40) histology shows H & E stained section with multiple fragments of soft tissue made up of heavily inflamed fibrous and granulation tissue. The lining epithelium is proliferative and non-keratinized. The fibrous and granulation tissue is heavily infiltrated by plasma cells, lymphocytes, neutrophils and macrophages.
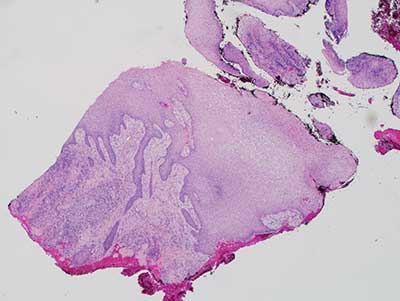
Figure 4 Low power (X40) histology shows H & E stained section with multiple fragments of soft tissue made up of heavily inflamed fibrous and granulation tissue lined by proliferative and keratinized surface epithelium with elongated rete pegs. The fibrous and granulation tissue is heavily infiltrated by plasma cells, lymphocytes, neutrophils and macrophages.
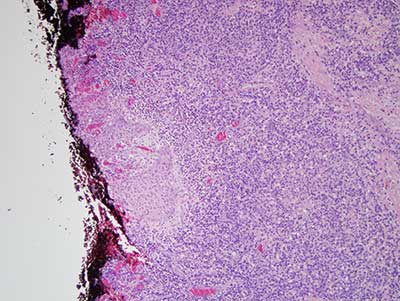
Figure 5 Higher power (X100) histology shows H & E stained section with multiple fragments of soft tissue made up of heavily inflamed fibrous and granulation tissue lined by non-keratinized epithelium infiltrated by neutrophils.
After you have finished reviewing the available diagnostic information