Expansile radiolucency, right posterior mandible
Can you make the correct diagnosis?
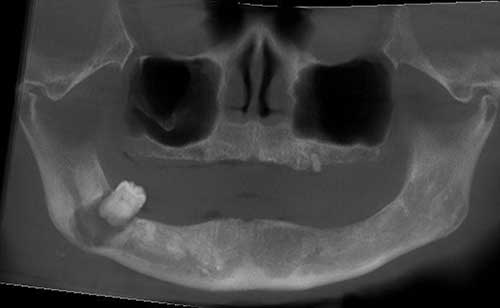
This is a 72-year-old male who visited his dentist with a chief complaint of pain in the right posterior mandible associated with the only intact tooth remaining in his mouth.
Sorry, you are incorrect!
The differential diagnosis (DDX) for an expansile radiolucency in the posterior mandible perforating bone should include ameloblastoma (especially the solid type) in a high position. Solid-type ameloblastoma usually presents as a multilocular expansile radiolucency, while the radiographic presentation in this case is unilocular radiolucency with a scalloped border. This presentation is less likely for a solid type of ameloblastoma and more likely for a unicystic ameloblastoma. Smaller and early developing solid ameloblastomas can present as unilocular radiolucencies, but less commonly. The older age of the patient is not typical of solid ameloblastoma; the mean age of occurrence is around 33-36 years of age with a range of the third to the sixth decade of life. The patient’s age is also not consistent with unicystic ameloblastoma, where the range of occurrence is around 10-20 years of age. The lack of association with an impacted tooth also contraindicates a diagnosis of unicystic ameloblastoma. Ameloblastomas tend to have no gender predilection. The severe periodontitis and periapical involvement demonstrated in Figure 1 is not consistent with the clinical and radiographic presentation of ameloblastomas. The patient’s pain in this case is attributed to infection and bone perforation, which is not specific to any one cyst or neoplasm. The histology in this case is not consistent with ameloblastoma, whether solid or unicystic.
Sorry, you are incorrect!
The differential diagnosis (DDX) list for an expansile radiolucent lesion in the posterior mandible perforating bone should also include odontogenic myxoma. This benign but locally aggressive neoplasm usually affects patients between 20 and 30 years of age; it occurs rarely in individuals older than 50 years of age. This patient is therefore on the much older side of the possible age spectrum, but odontogenic myxoma should remain on the DDX because such cases have nevertheless been reported. The unilocular radiolucency with a scalloped border can be consistent with a smaller developing odontogenic myxoma, but the larger neoplasms tend to be more multilocular and expansile. As stated in the discussion of ameloblastoma, the severe periodontitis and periapical involvement demonstrated in Figure 1 is also inconsistent with the clinical and radiographic presentation of odontogenic myxoma. Also, the patient’s pain is attributed to infection and bone perforation. The histology in this case is not consistent with odontogenic myxoma.
Congratulations, you are correct!
The severe localized periodontitis involving the apex of tooth #32 is a radiographic presentation consistent with combined periapical and periodontal pathosis. In this case, it is more likely that the severe periodontitis was the beginning of the disease process which eventually devitalized the tooth through trauma and infection. The unilocular expansile presentation is not typical of either of these pathologies, but has been described in association with periapical cysts and granulomas, especially when they are large and infected. The bone perforation is also unusual, but with severe inflammation, purulence and expansion can cause thinning and perforation of bone. The patient’s pain is also attributed to infection and bone perforation. The histology in this case is consistent with combined periapical and periodontal disease: specifically, the combination of a periapical cyst and periodontitis.
Sorry, you are incorrect!
A posterior mandible, unilocular radiolucency with a scalloped border associated with perforation of bone is a clinical and radiographic presentation that suggests that odontogenic keratocyst be considered on the differential diagnosis (DDX). The expansion is unusual since OKCs tend not to expand the jaw, but rather destroy bone in an anterior-posterior manner. However, larger OKCs can expand jaws. The age of this patient is on the older side of the typical age range since the biggest cluster of occurrences is between 20 and 40 years of age. The age range, however, is wide and can include patients under 10 and over 90 years of age. Pain, as in the other conditions in this differential diagnosis, is unusual for OKC but can be attributed to infection and bone perforation in this case. As stated before, the severe periodontitis and periapical involvement demonstrated in Figure 1 is not consistent with the clinical and radiographic presentation of OKC. The histology in this case is not consistent with odontogenic keratocyst.
Sorry, you are incorrect!
The clinical presentation of an expansile radiolucency perforating bone should bring to mind another aggressive cyst: glandular odontogenic cyst (GOC). This cyst, however, is more commonly described in the anterior mandible. That said, there are reports that indicate equal distribution between the anterior and posterior mandible. GOC is traditionally described in middle-aged patients, with a mean of 46 years of age and a range of the fourth to the seventh decades of life. This patient is therefore on the older side of the possible age range, but such cases have been described. While some studies report no significant gender predilection, others report a slight male predominance. The radiographic findings in this case are also consistent with GOC, which often resemble those of odontogenic keratocyst or ameloblastoma, the former presenting as a unilocular radiolucency with scalloped borders and the latter as a multilocular and expansile radiolucency. As stated before, the severe periodontitis and periapical involvement demonstrated in Figure 1 are not consistent with the clinical and radiographic presentation of GOC. The patient’s pain is attributed to infection and bone perforation. The histology in this case is not consistent with glandular odontogenic cyst.