Large, rough red & white lesion left posterior buccal mucosa/vestibule
Contributed by Greg Maggass, Jr., UWSOD 3rd year Dental Student
Dr. Michael Martin, Department of Oral Medicine Department, UWSOD, Seattle, WA
Case Summary and Diagnostic Information

This is a 51-year old white female who described her condition as follows: “There is a painful cyst on my gums on the lower left.”
This is a 51-year old white female who described her condition as follows: “There is a painful cyst on my gums on the lower left.” The patient reported being seen by her regular dentist two months ago; the dentist referred her to the UWSOD Department of Oral Medicine. The patient tried coconut oil pulling and various natural remedies that were not helpful. She has a 15-year history of widespread lichen planus involving several oral sites including the bilateral buccal mucosa, vestibules, and upper and lower lips. At presentation, the lesion (Figure 1) was diffuse, corrugated to verrucoid, and rough in consistency. There were areas of focal ulceration associated with a mild burning sensation and pain.
Figure 1 This photograph was taken at the first clinical presentation. Note the diffuse, papillary, red and white and ulcerated lesion at the left posterior buccal mucosa and vestibule.
The patient’s past medical history is significant for toxic mold exposure 16 years ago, a 15-year history of lichen planus, high cholesterol, fibromyalgia, two C-section surgeries in 1990 and 1992, and a hysterectomy in 2002. She also has a history of hypersensitivity to sulfa drugs.
The left buccal mucosa was diffusely red and white with surface ulceration and papillary configuration (Figure 1). The computed tomography (CT) imaging measured this lesion at 2.5 X 1.6 X 1.6 cm in greatest dimensions infiltrating the alveolar bone in area of tooth #18 (Figure 2). The CT imaging also showed multiple enlarged lymph nodes in the area, one was larger than on cm (Figure 3). The soft tissue mass involved the posterior buccal mucosa and with deep vestibular extension. The lesion was rough to palpation and was verrucoid. It was painful as described by the patient with focal ulceration.
Figure 1 This photograph was taken at the first clinical presentation. Note the diffuse, papillary, red and white and ulcerated lesion at the left posterior buccal mucosa and vestibule.
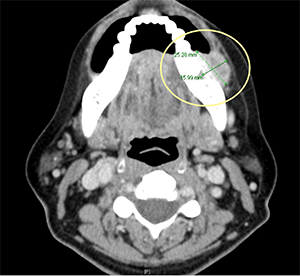
Figure 2 This image represents an axial cut of a contrast-enhanced computed tomogram. It shows a soft tissue mass adjacent to tooth #18 within the buccal vestibule measuring 2.5 x 1.6 x 1.6 cm. It appears to be eroding into the alveolar ridge around tooth #18.
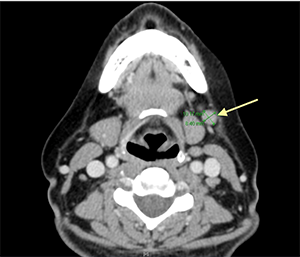
Figure 3 This image represents an axial cut of a contrast-enhanced computed tomogram. It shows a well-demarcated round mass (arrow) located along the side of the neoplasm in the vestibule measuring 1.2 X 0.84 X 1.2 cm. It represents a large lymph node. There are more enlarged lymph nodes in this area.
Under local anesthesia, the buccal mucosa was biopsied using a 5mm punch biopsy and submitted for microscopic examination. The area healed within a short period of time. Based on the results of the incisional biopsy, the patient was referred for further definitive treatment.
Histologic examination revealed a small piece of soft tissue composed of surface epithelium exhibiting high grade atypia invading the underlying fibrous connective tissue (Figures 4-5). The epithelial atypia is manifested in loss of maturation, alteration in the nuclear/cytoplasmic ration, individual cell keratinization and nuclear pleomorphism. The neoplastic epithelial cells invade the connective tissue in form of nests and small islands (Figures 4-5).
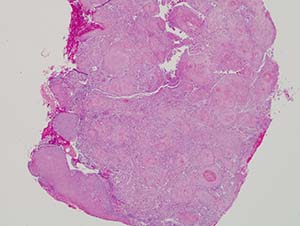
Figure 4 Scan power (x40) H & E stained section reveals a small fragment of oral mucosa with papillary proliferation of neoplastic cells cut tangentially. Invasion is present in multiple areas in form of small nests and islands. The neoplastic cells show evidence of loss of maturation, mitotic activity, nuclear pleomorphism, hyperchromatism and individual cell keratinization.
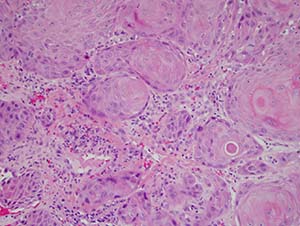
Figure 5 High-power (x200) H & E stain section reveals a closer look at the neoplastic epithelial cells invading the connective tissue.
After you have finished reviewing the available diagnostic information