Left maxilla: mixed RL/RO swelling
Contributed by Dr. Mathew Epstein
Greenlake Facial Surgery, Seattle, WA
Case Summary and Diagnostic Information

This is a 13-year-old female who was referred in 2015 for the management of a palatally impacted tooth #12.
This is a 13-year-old female who was referred in 2015 for the management of a palatally impacted tooth #12. The tooth was exposed and orthodontically guided into the alveolar arch with the aid of a temporary anchorage device. In May 2017, the patient returned with a swelling in the left posterior maxilla. The CBCT revealed a large well-defined mixed radiolucent and radiopaque mass in the left maxilla extending into the left maxillary sinus (Figures 1 & 2). The mass was 2.8 x 2.2 x 2.2 cm in size. There was no perforation of bone, but the roots of tooth #13 were displaced. On clinical evaluation, the left maxillary vestibule was asymmetrical. The patient reported she had noticed the change slowly occurring over the past two years.
Figure 1 This is a CBCT panoramic view demonstrating a large, well-circumscribed radiolucent/radiopaque lesion in the left posterior maxilla mandible extending into the left maxillary sinus.

Figure 2 This is a closer CBCT radiographic image of the large and well-circumscribed radiolucent/radiopaque lesion in the posterior maxilla and left maxillary sinus.
The past medical history is significant for tonsil and adenoid removal and hypersensitivity to penicillin.
This patient was first referred in 2015 for the management of an impacted tooth #12. The tooth was exposed and orthodontically guided into the alveolar arch with the aid of a temporary anchorage device. The patient noticed a gradual change over a two-year period. In May 2017 the patient returned with no perceptible movement of tooth #12. A CBCT was obtained which revealed a large, well-circumscribed, and homogeneous mixed radiolucent/radiopaque lesion in the left posterior maxilla extending into the left maxillary sinus (Figures 1 & 2). The mass was expansile but did not perforate bone. Clinically, the left maxillary vestibule was asymmetrical when compared to the contralateral side.
Incisional biopsy: Under IV sedation, tooth # 12 was extracted and a biopsy was obtained at the same time. On elevating a buccal flap, the alveolar cortical bone was observed to be extremely thin. The alveolus was entered with a curette and a large amount of spongy tissue was removed.
Excisional surgery: Under IV sedation, the remaining lesion was curetted and the area re-contoured.
Histologic examination revealed multiple pieces of decalcified hard and soft tissue composed of a benign fibro-osseous lesion made up of cellular connective tissue stroma containing calcified cementum-like globules and small bony trabeculae with feathery edging. The connective tissue stroma is moderately cellular, composed of short strands of spindle-shaped cells suspended on delicate collagen fibers. The cementum-like globules are of variable shapes and sizes.
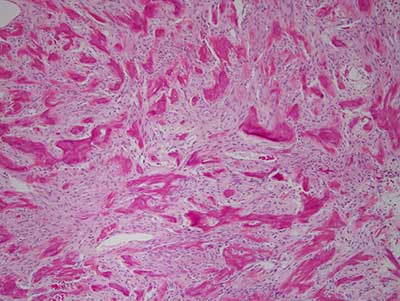
Figure 3 This is a low power (100X) micrograph of an H & E stained section, representing a decalcified fragment of benign fibro-osseous lesion with small bony and cementum like hard tissue suspended on moderately cellular connective tissue stroma.
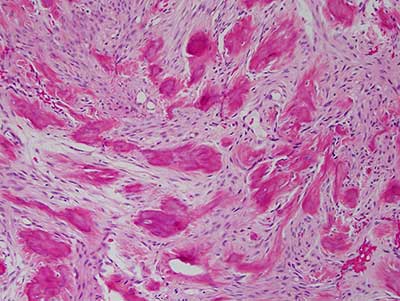
Figure 4 This is a higher power (200X) micrograph of an H & E stained section demonstrating the benign fibro-osseous lesion composed of bone and cementum-like hard tissue suspended on moderately cellular connective tissue stroma.
After you have finished reviewing the available diagnostic information