August 2016: Gingival swelling, lingual gingiva between teeth #s 24 & 25s
Contributed by Dr. Fred Farhat
Seattle, WA
Case Summary and Diagnostic Information

This is a 64-year-old male who presented with a painful, mostly smooth-surfaced pink gingival swelling.
This is a 64-year-old male who presented with a painful, mostly smooth-surfaced pink gingival swelling. It was similar to the surrounding tissue except focally, where surface ulceration was noted. It was present lingual to and between teeth #s 24 and 25 (Figure 1). The swelling was slow growing. It had presented two years earlier and had been conservatively excised in 2014, but it recurred in the same site, growing at a faster rate than previously. Radiographically, there is evidence of moderate horizontal bone loss (Figure 2) that includes other parts of the mouth (generalized). Tooth mobility was also noted.
Figure 1 This photograph is taken at the first clinical presentation. The figure shows a swelling that is smooth surfaced and pink with a small area of surface ulceration. The swelling is present lingual and between teeth # 24 and 25. Note the excessive calculus and external stain to the teeth.
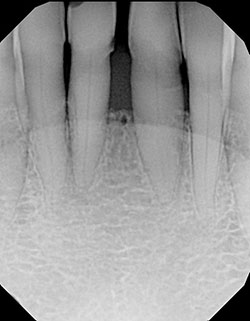
Figure 2 This radiograph is taken at the first clinical presentation. The figure shows moderate horizontal bone loss involving the anterior incisors and lateral teeth.
This patient’s past medical history is significant for leiomyosarcoma of the extremities diagnosed in 1984. In 2013, he presented with high-grade leiomyosarcoma of the right kidney, liver and the regional lymph nodes. Treatment included surgery and multiple courses of chemotherapy and immunotherapy. In 2014, he presented with a single gingival swelling lingual to teeth #s 24 & 25 which was conservatively excised. The lesion recurred recently in the same site and was again conservatively excised.
The oral gingival swelling was slow-growing and painful which was removed in 2014. The area healed with no evidence of recurrence for two years. The current lesion presented in the same site and was similar in size and color to the previous lesion, but was faster growing and was associated with tooth mobility and increased diastema between teeth #s 24 & 25.
Under local anesthesia the swelling was conservatively removed to improve symptoms. Using an internal bevel incision, the lesion was excised with 1-2mm of clear margins. The area was sutured with 5/0 gut and the specimen was submitted for microscopic evaluation. Chlorhexidine rinses were prescribed.
Histologic examination of both specimens (2014 1nd the current) reveals multiple pieces of soft tissue composed of a neoplasm of spindle cell origin (Figures 3 & 4). This neoplasm is covered by thin but well differentiated layer of mature surface epithelium. The neoplasm is made up of spindle-shaped cells crisscrossing each other in long bundles. The neoplastic cells show evidence of pleomorphism and nuclear hyperchromatism (Figure 4). There is also evidence of high mitotic activity, some of which are atypical. There is evidence of focal necrosis. The histology is similar to that of the same neoplasm removed from the kidney in 2013. The kidney tumor shows <50% tumor necrosis and 21 mitoses in 10 HPF`s. By immunohistochemistry staining, the neoplastic cells of both the oral and the kidney tumors are uniformly positive with antibodies to smooth muscle actin and desmin (Figures 5 & 6).
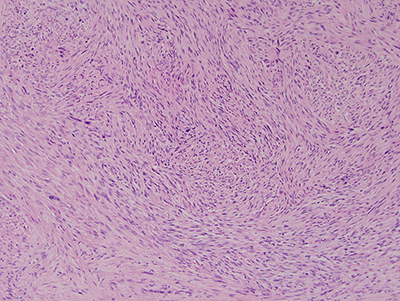
Figure 3 Low power (X100) H & E stained section revealing a cellular soft tissue mass made up of spindle-shaped cells arranged in long bundles crisscrossing each. The neoplastic cells show evidence of pleomorphism and mitotic activity.
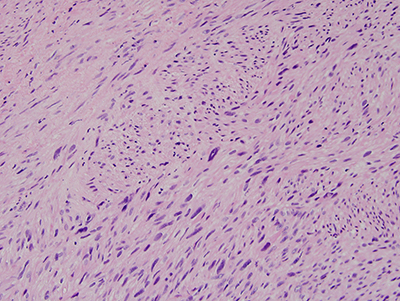
Figure 4 Higher power (X200) H & E stained section revealing a closer look at the spindle-shaped neoplastic cells with evidence pleomorphism and mitotic activity
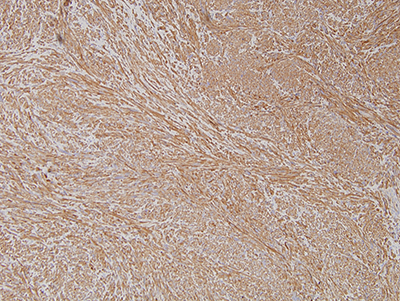
Figure 5 Higher power (X100) Immunohistochemistry stain with antibody to smooth muscle actin (1A4) revealing a cellular soft tissue mass uniformly positive for smooth muscle actin.
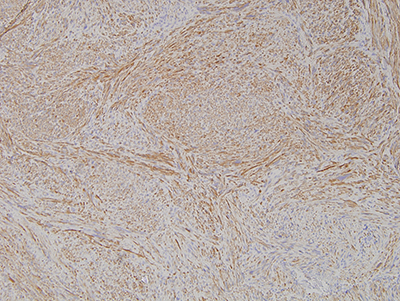
Figure 6 Higher power (X100) Immunohistochemistry stain with antibody to muscle desmin revealing a cellular soft tissue mass uniformly positive for this antibody.
After you have finished reviewing the available diagnostic information