All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Ulcerated gingival swelling between teeth #s 24 & 25
Contributed by:
Dr. Brian Brancheau
Periodontics & Implants, Lynnwood, WA
Case Summary and Diagnostic Information
This is an 85-year-old male who presented with an ulcerated gingival swelling between teeth #s 24 & 25 of three weeks duration.

This is an 85-year-old male who presented with an ulcerated gingival swelling between teeth #s 24 & 25 of three weeks duration. This swelling involved the buccal and lingual gingiva (Figures 1 & 2). Teeth around this swelling showed class III mobility and about 8-10 mm periodontal depths. Radiographically, there is evidence of moderate horizontal bone loss (Figure 3). The patient denied pain or sensitivity in the area. His dentist prescribed chlorhexidine mouthwash and Amoxicillin with no change. Patient was referred for an incisional biopsy of the area.
Figure 1 This photograph is taken at the first clinical presentation. The figure shows an ulcerated and red gingival swelling; buccal gingiva between teeth #s 24 and 25.

Figure 2 This photograph is taken at the first clinical presentation. The figure shows an ulcerated gingival swelling covered by a thick layer of pseudomembrane; lingual gingiva between teeth #s 24 and 25.

Figure 3 This radiograph is taken at the first clinical presentation. The figure shows moderate horizontal bone loss involving the anterior mandible, area of teeth #s 23-26.
This patient’s past medical history is significant for high blood pressure, prostate disease, respiratory illness, malignant pleural mesothelioma and mild dementia.
The gingival swelling was of three weeks duration but not painful. It was ulcerated and involved the buccal and lingual gingiva. It was large about 15 X 10 mm in greatest length and width dimension (Figures 1 & 2). Patient also had multiple small white lesions in the floor of the mouth measuring 3 X 3 mm. Periodontal exam revealed class III mobility of teeth #24 and 25 with 8-10mm PDs. A periapical x-ray shows moderate horizontal bone loss in area of teeth #s 23-26 (Figure 3)
Under local anesthesia using one carpule 2% Lidocaine infiltration, incisional biopsy with 15c was performed. Buccal gingiva was biopsied 5x5mm size. No sutures were needed. The biopsy specimen was submitted in formalin to for microscopic examination.
Histologic examination reveals a piece of soft tissue composed of a neoplasm madeup of spindle-shaped and epithelioid cells with ulcerated surface and focal necrosis (Figure 4 & 5). The spindle-shaped and epithelioid cells show evidence of high-grade atypia and high mitotic activity. The cellular atypia is manifested in nuclear hyperchromatism and pleomorphism. The immunohistochemistry (IHC) stain is diffusely positive with CK5 (Figure 6) and was negative with p40 (Figure 7) arguing against squamous cell carcinoma, The IHC stain was positive with antibody to D2-40 (Figure 8), and focally positive with calretinin (Figure 9). The IHC stain is negative WT1. All six controls were appropriately positive
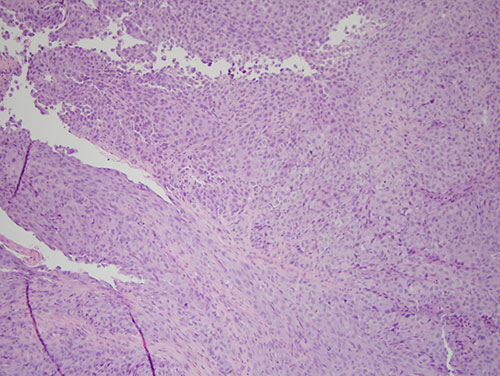
Figure 4 Low power (X40) H & E stained section revealing a cellular soft tissue mass made up of spindle-shaped and epithelioid cells with ulcerated surface.
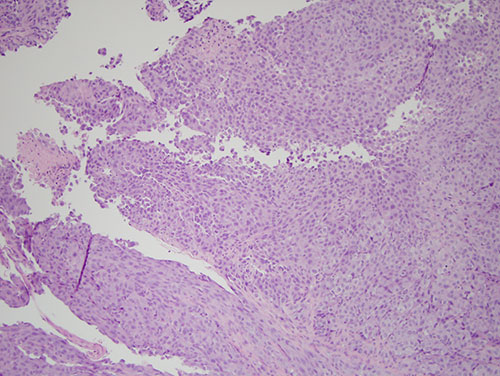
Figure 5 Higher power (X100) H & E stained section revealing a closer look at the spindle-shaped and epithelioid neoplastic cells
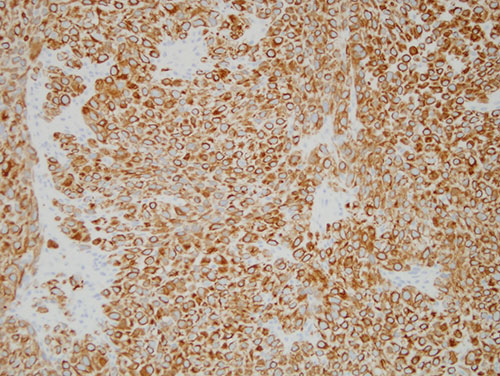
Figure 6 Higher power (X200) Immunohistochemistry stain with antibody to CK5 cytokeratin revealing uniform positive stain.
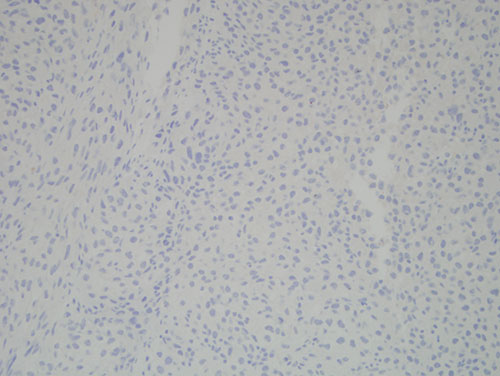
Figure 7 Higher power (X200) Immunohistochemistry stain with antibody to p40 revealing negative results arguing against these cells being squamous cell carcinoma.
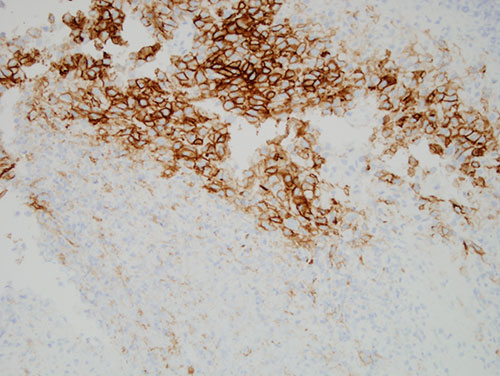
Figure 8 Higher power (X200) Immunohistochemistry stain with antibody to D2-40 revealing patchy positive staining.
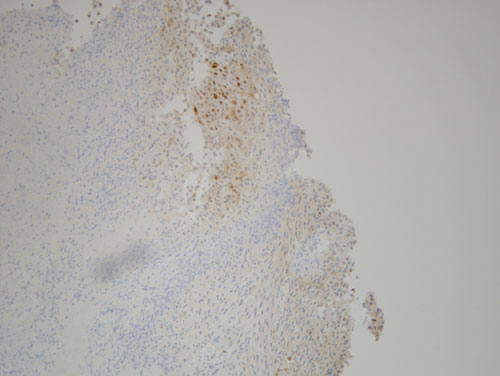
Figure 9 Higher power (X200) Immunohistochemistry stain with antibody to caltrenin revealing focal positive staining.
After you have finished reviewing the available diagnostic information