Large & Well-Demarcated Radiolucency Left Posterior Mandible
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by: Dr. Michael Medley
Oral & Maxillofacial Surgery, Olympia, WA
Case Summary and Diagnostic Information
This is a 21-year-old white female with a four-month history of radiolucency in the left posterior mandible.
Diagnostic Information Available
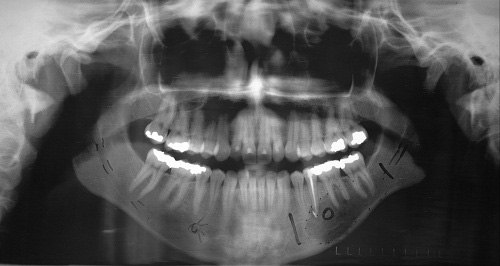
This is a 21-year-old white female with a four-month history of radiolucency in the left posterior mandible (Figure 1). This condition started with pain in the area which was interpreted to be endodontically related. Thus, tooth #20 was treated. The patient’s past medical history is unremarkable.
Figure 1. This is a panoramic radiograph taken at first clinical presentation. Note the large, well-defined unilocular radiolucency involving area of teeth #s 18-21.
The patient’s past medical history is negative for any significant diseases or risk factors.
The patient reported pain in the left mandible that was related to tooth #20 and was endodontically treated. The pain and the radiolucency persisted for about four months.
Treatment
Under local anesthesia, a full-thickness flap around the area was raised and the area was curetted. The area was sutured and the specimen submitted for microscopic evaluation.
Excisional Biopsy
Histologic examination reveals multiple pieces of decalcified hard and soft tissue composed of bone and sheets and nests of cells with granular cytoplasm (Figure 2). The latter cells comprise the bulk of the soft tissue and are round-to-oval eosinophilic cells with abundant granular eosinophilic cytoplasm and round nuclei. These cells are arranged in sheets and small nests with alveolar and organoid architecture in some areas (Figure 3). These cells are surrounded by connective tissue septae with prominent vascularity as clearly demonstrated by 1A4 antibody. The neoplastic cells are uniform in morphology and show no evidence of mitotic activity or atypia. There is no evidence of remnants of odontogenic epithelium or calcifications. Also present is bone which comprises a significant portion of the specimen and is both reparative and lamellar in type. It contains viable osteocytes and reversal lines. The special stain with PAS-diastase demonstrates intracytoplasmic granules. The specimen was stained with immunohistochemistry, a total of thirteen antibodies including AE1/AE3, PAX2 and RCC, Thyroglobulin, Chromogranin and Synaptophysin, S-100 and Cd1a; these were all negative. There was a rare positive staining with desmin combined with uniform positive staining with TFE3 (Figure 4) and CD44.
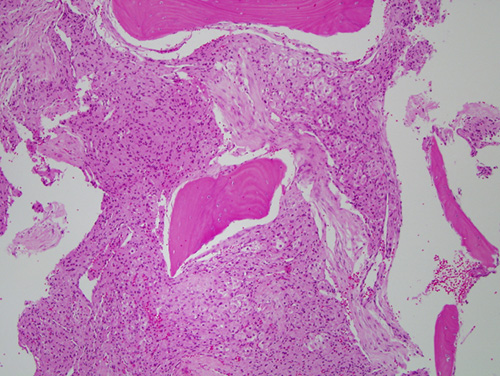
Figure 2. Low power (x100) H & E histology illustrates sheets and nests of cells with granular cytoplasm. The cells are round to oval with abundant granular eosinophilic cytoplasm and round nuclei. Some of these cells are arranged in sheets and others in small nests with alveolar and organoid morphology.
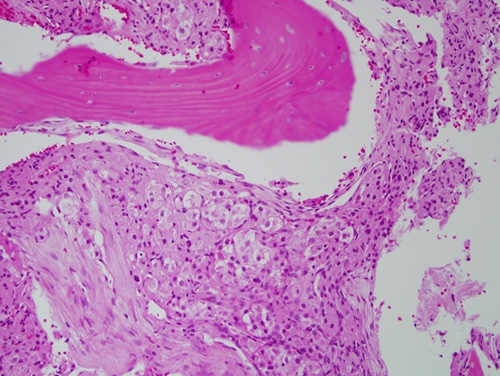
Figure 3. Higher power (x200) H & E histology illustrates nests of cells with eosinophilic granular cytoplasm arranged in an alveolar and organoid pattern.
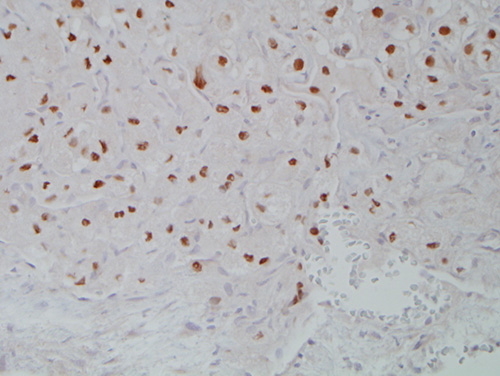
Figure 4. Higher power (x200) Immunohistochemistry staining with uniform positive staining with TFE3.
After you have finished reviewing the available diagnostic information