Mixed Radiolucent Radiopaque Lesion Associated with Impacted Tooth #14
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by: Dr. Libby Kutcipal
Seattle Children’s Hospital and Center for Pediatric Dentistry, Seattle, WA
Case Summary and Diagnostic Information

This is a 7-year-old female who first presented to the Center for Pediatric Dentistry with a chief complaint of pain associated with cracked tooth #D.
Diagnostic Information Available
This is a 7-year-old female who first presented to the Center for Pediatric Dentistry with a chief complaint of pain associated with cracked tooth #D. During the oral examination to find the source of the pain, it was discovered that tooth #14 was missing while all the other three first molar teeth had erupted (Figure 1). The panoramic radiograph demonstrates an impacted tooth #14 surrounded by a large radiolucent/radiopaque lesion which was otherwise asymptomatic; there was no pain or parasthesia. Clinical examination of the area showed an expansion at the left maxilla overlying the lesion.
Figure 1. This is a panoramic view of the area taken at the initial presentation. Note the impacted/unerupted tooth #14 surrounded by a radiolucent/radiopaque lesion.
The patient’s past medical history is otherwise unremarkable.
This lesion was discovered during an oral examination related to painful tooth #D. The patient’s pediatric dentist noticed the only unerupted first molar and discovered a swelling in the area. The panoramic radiograph demonstrated a large mixed radiolucent/radiopaque lesion associated with the crown of tooth #14 (Figure 1). The patient was referred to a pediatric oral surgeon for further workup and treatment.
Figure 1. This is a panoramic view of the area taken at the initial presentation. Note the impacted/unerupted tooth #14 surrounded by a radiolucent/radiopaque lesion.
Treatment
The decision was made to perform an excisional biopsy of the lesion under intravenous general anesthesia. Induction of anesthesia was performed by the anesthesia team. Throat pack was placed and a sulcular incision around the tooth was made and carried back to the tuberosity with a distobuccal releasing incision. The lesion was removed in its entirety and submitted in formalin for histopathologic review. The surgical site was irrigated and closed with 3-0 chromic gut. Throat pack was removed.
Excisional Biopsy
Histologic examination reveals multiple pieces of hard and soft tissue embedded in three separate blocks labeled A1-A3. All specimens are composed of a neoplasm of mixed odontogenic origin (Figures 2-4). The bulk of the specimen is made up of connective tissue stroma with epithelial islands. The epithelial islands are of variable shapes and sizes (Figures 2-3) and the fibrous connective tissue stroma is loose and myxoid with spindle-shaped or stellate fibroblasts suspended on delicate collagen fibers (Figures 2-3). The specimen also contains areas of hyalinized connective tissue and areas of calcified material. The latter is mostly cementum and dentin-like material (Figure 4).
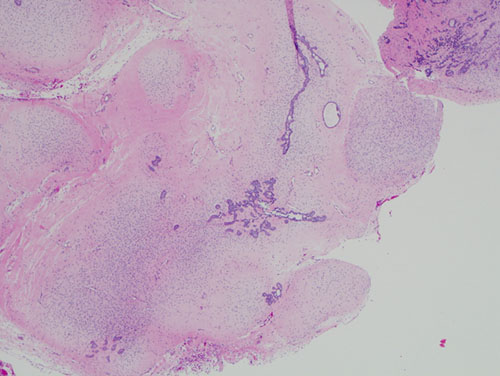
Figure 2. Low power (x40) H & E histology shows mixed epithelial and odontogenic neoplasm composed of primitive connective tissue stroma with odontogenic epithelial islands, cords and rosettes of variable shapes and sizes.
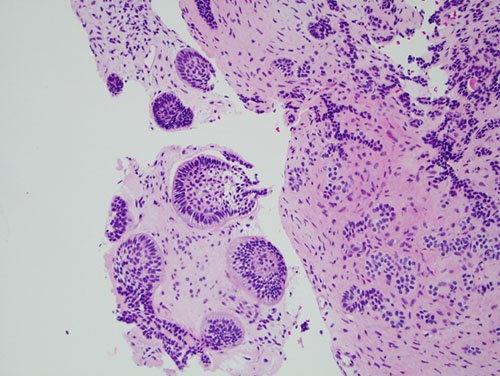
Figure 3. Higher power (x200) H & E closer look histology demonstrating the epithelial islands some with palisaded cuboidal/columnar cells at the periphery and spindle-shaped to cuboidal epithelial cells in the center of the islands.
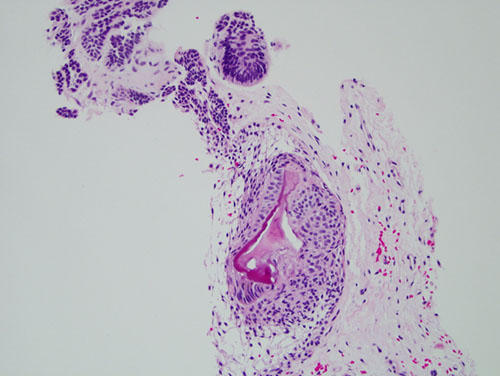
Figure 4. High power (x400) H & E histology shows calcified odontogenic material being produced by the neoplastic odontogenic epithelial cells.
After you have finished reviewing the available diagnostic information