Return to Case of the Month Archives
September 2010: Multiple Radiolucencies of the Maxilla and Mandible
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Michael Werner
South Sound Oral Surgery, Olympia, WA
Case Summary and Diagnostic Information
This is a 14-year-old white male who was referred to South Sound Oral Surgery by his general dentist for extraction of a painful, carious mandibular left first molar.
Diagnostic Information Available
This is a 14-year-old white male who was referred to South Sound Oral Surgery by his general dentist for extraction of a painful, carious mandibular left first molar. A panoramic radiograph taken by the dentist revealed four large cystic lesions (Figure 1). The first was associated with impacted tooth #4; the second with impacted tooth #11; the third with impacted tooth #17, displacing tooth #18; and the fourth with impacted tooth #32. Teeth #s 17 and 32 were displaced vertically into the superior ramus. There was a hint of scalloping associated with the radiolucencies in the areas of teeth #s 17 & 32, especially with tooth #17. The latter area also showed evidence of buccolingual expansion but no other area exhibited expansion. The patient’s past medical history is positive for a ventriculoperitoneal shunt which had been in place and functioning well for many years. He was hospitalized for pneumonia December 1999, at which time the chest x-ray revealed bifid right third and fourth ribs and broadening of the lateral aspect of the third rib with partial fusion of the fifth and sixth ribs.
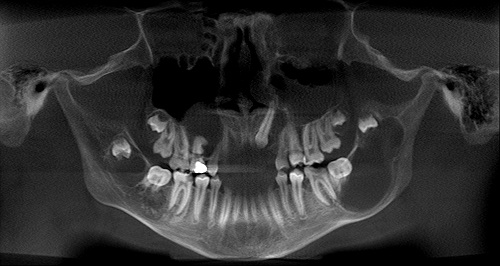
Figure 1 Panoramic view at first presentation demonstrating a total of four cysts, area of teeth #s 4, 11, 17 and 32. The cyst associated with tooth #17 is the largest radiolucency which is has a scalloped border.
The patient’s past medical history includes orthodontic treatment of one year’s duration during which time there was little or no movement of teeth. He has no allergies and is not on any medications. There is no family history of related disease.
Clinical examination revealed mild buccolingual swelling in the left posterior mandible (Figure 1) but otherwise neither jaw showed evidence of any significant change. The patient presented with pain in the left posterior mandible, but the pain was related to a badly carious tooth #18 and not to the large cyst behind this tooth. Radiographic findings were striking (Figure 1). There were a total of four radiolucencies, two in the maxilla and two in the mandible. The two in the maxilla were unilocular radiolucencies around impacted teeth #s 4 and 11. One of the two cysts present in the mandible was a unilocular radiolucency with a scalloped border associated with tooth # 17 and extending into the ramus; the other was a large unilocular radiolucency associated with tooth #32. In addition, the patient shows evidence of few palmar pits (Figure 2) which are usually not common in children.
Figure 1 Panoramic view at first presentation demonstrating a total of four cysts, area of teeth #s 4, 11, 17 and 32. The cyst associated with tooth #17 is the largest radiolucency which is has a scalloped border.

Figure 2 This photographs demonstrates the presence of a few palmar pits which are usually not common in children but tend to be more evident in individuals with manual labor.
Treatment
Under general anesthesia, the patient underwent excision and peripheral ostectomy of all four cysts. Teeth # 4,11,17,18, 19, 30, 31, and 32 were extracted as the cystic lesion was adherent to and had eroded into the bifurcation areas of all the first and second molars. There were two discrete 5mm areas in the mandibular right where the cyst had eroded into the inferior alveolar canal exposing the nerve, but no areas of frank bony buccal or lingual perforation. The patient reported no paresthesia postoperatively.
Incisional Biopsy
Histological examination of specimens from the area of teeth #s 4, 11, 17/18 and 32 revealed that all of them were similar. They were all made up of cystic structures (Figure 3). All cystic structures were lined by keratinized stratified squamous epithelium and supported by connective tissue walls. The lining epithelium was uniformly thin, corrugated and covered by parakeratin. The basal cell layer was palisaded (Figure 4). The lumen of some of the cysts was filled with keratin (Figure 5). The connective tissue wall was lose and cellular in some areas and fibrotic in others.
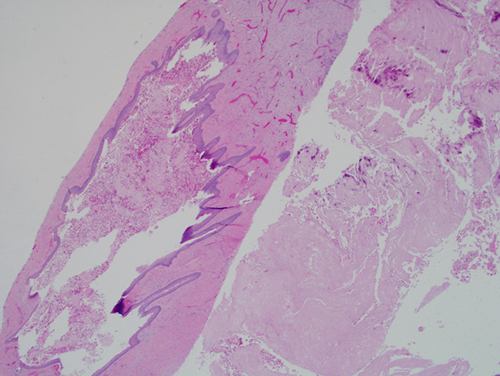
Figure 3 Higher power (x100) H & E histology shows a cystic structure with lining epithelium and a supporting fibrous connective tissue wall. The lining epithelium is uniformly thin and is corrugated and keratinized with palisaded basal cell layer. Note layers of keratin associated with this cyst.
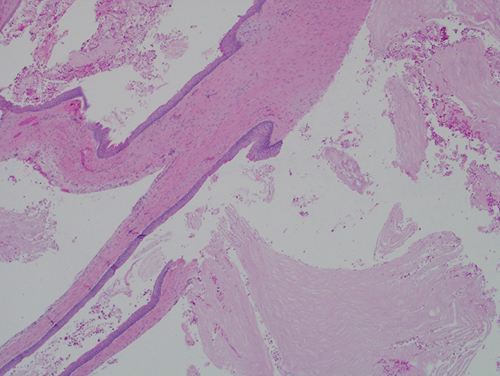
Figure 4 Low power (x200) H & E closer look histology shows a cystic structure with keratinized lining epithelium and palisaded basal cell layer. Note the layers of keratin fibers associated with this cyst.
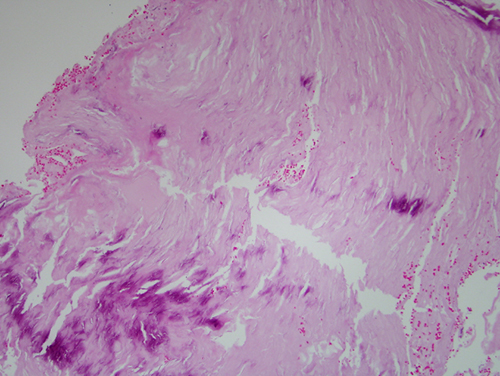
Figure 5 Higher power (x200) H & E closer histology of the layers of keratin with focal areas of early calcification.
After you have finished reviewing the available diagnostic information