Return to Case of the Month Archives
September 2007: Multilocular expansile radiolucency of the left posterior mandible
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Jon Crawford, Columbia Basin Oral & Maxillofacial Surgeons
Kennewick, WA
Case Summary and Diagnostic Information
This 51-year-old white male was referred by his general dentist in May 2007 for obvious mandibular asymmetry along the inferior border of the left mandible.
Diagnostic Information Available
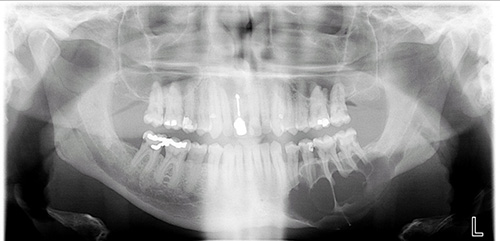
This 51-year-old white male was referred by his general dentist in May 2007 for obvious mandibular asymmetry along the inferior border of the left mandible. The patient reported that the lesion had been there for at least 1 ½ years. He was vague as to why no biopsy or treatment had been rendered up to that point. At presentation, he was experiencing pain and periodic numbness in the left lip and chin. The panoramic radiograph showed a large multilocular and expansile radiolucency in the left posterior mandible involving most of the body of the mandible (Figure 1). The expansion involved the inferior border of the mandible, as well as the buccal alveolar ridge. The patient’s past medical history is significant for Crohn’s disease and tobacco use.
Figure 1. This panoramic radiograph is taken at first presentation. Note the large expansile multilocular radiolucency involving most of the body of the mandible.
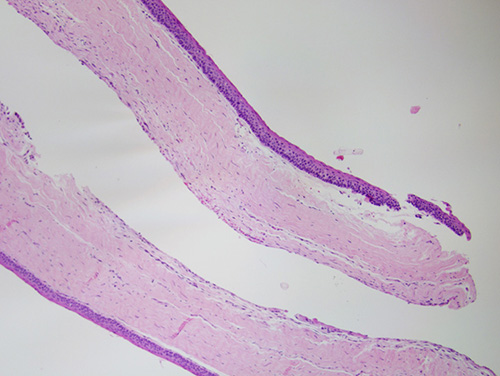
Figure 2. Low power (x100) histology shows a two fragments of a cystic structure lined by uniformly thin and keratinized stratified squamous epithelium and supported by fibrous connective tissue wall.
The patient’s past medical history is significant for Crohn’s disease and tobacco use. He also reports hypersensitivity reaction to penicillin and intolerance to a number of other antibiotics.
At presentation, the patient was not in any acute distress. He had obvious mandibular asymmetry with increased fullness along the inferior buccal alveolar ridge. An oral exam noted an intact dentition with multiple carious teeth, though these were firm and not mobile. No submandibular adenopathy was noted. A firm, non-tender, non-fluctuant swelling was noted in the buccal vestibule extending from the left angle of the mandible to the left parasymphysis area. In addition, a firm fullness was noted on the lingual left mandibular alveolar ridge. His oral hygiene was fair. Both the panoramic and CT scan demonstrated a large multilocular radiolucency of the left mandible with possible lingual bony perforation.
Histologic evaluation revealed two fragments of soft tissue made up of a cystic cavity lined by thin and keratinized stratified squamous epithelium supported by fibrous connective tissue wall (Figure 2). The lining epithelium is covered by parakeratin and is corrugated. The basal cell layer is palisaded (Figure 3) and the spinous layer is uniformly thin (Figures 2 & 3).
Figure 2. Low power (x100) histology shows a two fragments of a cystic structure lined by uniformly thin and keratinized stratified squamous epithelium and supported by fibrous connective tissue wall.
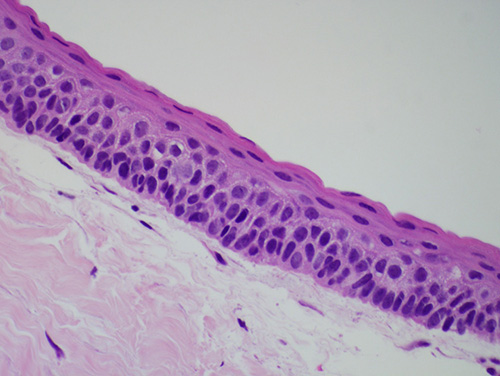
Figure 3. High power (x400) histology of the cystic structure shows palisaded basal cell layer; the spinous layer is of uniform thickness and the surface is corrugated and keratinized.
After you have finished reviewing the available diagnostic information