Partially Corticated, Expansile & Destructive Radiolucency Between Teeth #s 28 & 30
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by Dr. Adrian Pawlowski
Perio Innovations, Seattle, WA
Case Summary and Diagnostic Information
This is a 53-year-old Asian female who presented with an expansile and well-demarcated radiolucency involving teeth #s 28 & 30 of 18 months’ duration.
Diagnostic Information Available
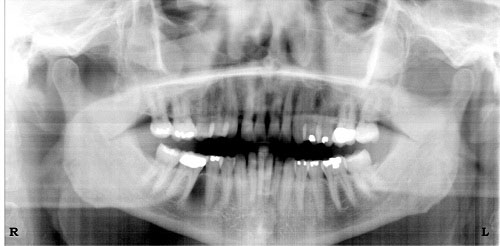
This is a 53-year-old Asian female who presented with an expansile and well-demarcated radiolucency involving teeth #s 28 &30 (Figures 1 & 2) of 18 months’ duration. The panoramic radiograph indicates a partially corticated and otherwise well-defined unilocular radiolucency with a second, more radiolucent destruction in the superior area between teeth #s 29 & 30. The latter area corresponded to buccal and lingual bone perforation. Teeth #s 28-30 were vital. Clinically, the lesion is described to be around 3.5-4 cm in size.
Figure 1. This is a panoramic radiograph taken at first clinical presentation. Note the partially corticated unilocular radiolucency in some areas and well-defined radiolucency in other areas all involving teeth #s 28-30. Also note the more radiolucent small round lesion superior and between teeth #s 29 & 30 indicating bone perforation.

Figure 2. This is a panoramic radiograph taken at first clinical presentation. It provides a closer look at the unilocular radiolucency and the perforation of bone between teeth #s 29 & 30.
The patient’s past medical history is negative for any significant disease or risk factors.
The patient reported progressive swelling of the right posterior mandible of unknown duration. The involved teeth were all vital. The swelling had perforated the buccal and lingual plates.
Treatment
Under local anesthesia, a full-thickness flap around the area was raised and the lesion enucleated in one piece (Figure 3) and the cavity was thoroughly curetted as shown in the composite Figure 3. The area was sutured and the specimen submitted for microscopic evaluation.
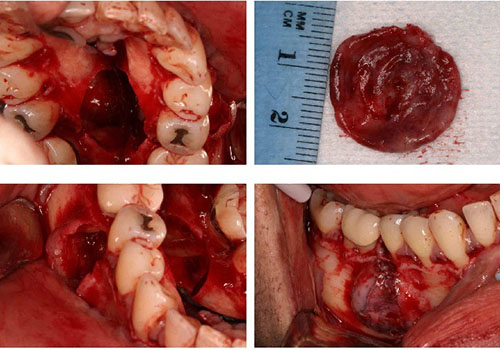
Figure 3. This is a composite figure representing the surgical flap followed by the clinical appearance of the lesion after the bone was exposed, followed by enucleation of the lesion which was removed intact in one piece.
Excisional Biopsy
Histologic examination reveals a multisected piece of soft tissue composed of a cystic structure lined by epithelium and supported by a fibrous connective tissue wall (Figures 4-6). The lining epithelium is uniformly thin and is slightly corrugated. It is covered by parakeratin. Some of the latter is present in the lumen of the cyst. The basal cell layer is focally palisaded (Figure 6). The connective tissue wall is fibrotic and thin in most parts. It is focally infiltrated by a few lymphocytes and plasma cells.
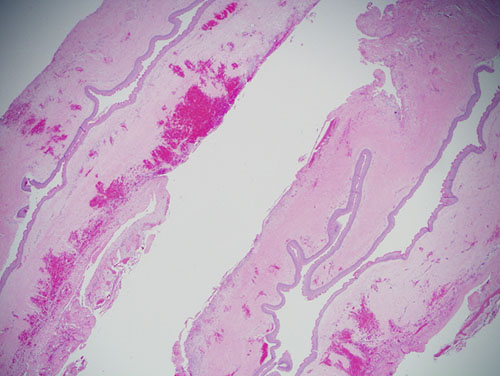
Figure 4. Low power (x40) H & E histology illustrates a cystic structure lined by keratinized stratified squamous epithelium supported by connective tissue wall.
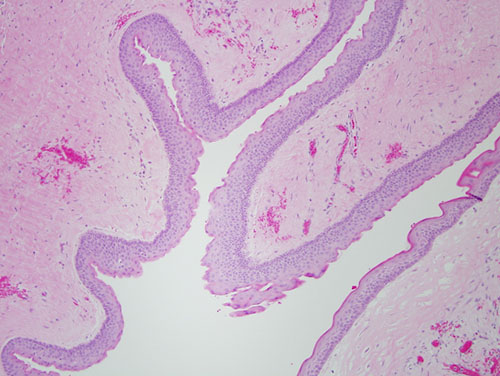
Figure 5. Higher power (x200) H & E histology illustrates a higher power of the cyst lining epithelium where it is corrugated and covered by a thin layer of parakeratin.
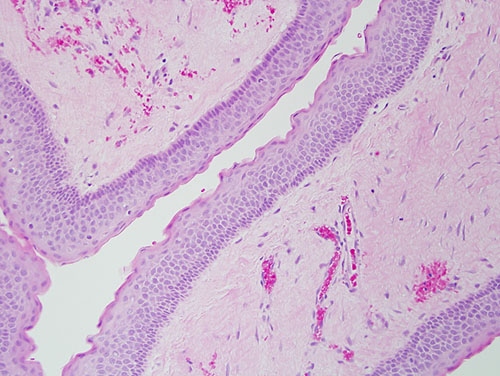
Figure 6. Higher power (x200) H & E histology illustrates a higher power of the lining epithelium demonstrating a palisaded basal cell layer.
After you have finished reviewing the available diagnostic information