Ill-defined Radiolucency, Anterior Mandible
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by: Dr. John Evans
Department Oral & Maxillofacial Surgery, University of Washington, Seattle, WA
Case Summary and Diagnostic Information

This is a 58-year-old male who was referred by his dental hygienist for evaluation of an anterior mandible midline bony lesion that had been present for several months.
Diagnostic Information Available
This is a 58-year-old male who was referred by his dental hygienist for evaluation of an anterior mandible midline bony lesion that had been present for several months. The patient had noticed loosening in his anterior mandibular teeth six months prior. He also reported a recent infection in the area that had been treated with antibiotics. At presentation, the area was swollen but not infected and the anterior mandibular teeth demonstrated 3+ mobility. Periapical radiographs demonstrated an ill-defined radiolucency with displaced teeth (Figures 1 & 2). The teeth were otherwise vital.
Figure 1. This radiograph was taken in first clinical presentation. Note the ill-defined radiolucency involving multiple teeth in the anterior mandible.

Figure 2. This radiograph was taken in first clinical presentation. Note the ill-defined radiolucency involving multiple teeth in the anterior mandible.
The patient’s past medical history is non-contributory but has a family history of kidney and liver disease.
The patient reported loosing of the anterior mandibular teeth over a six month period. He also reported a recent infection in the area that had been treated with antibiotics. Although the disease progressed, the involved teeth were vital but mobile. The mobility of teeth was localized to this area only making it unusual for periodontitis.
Treatment
After the excisional biopsy, the patient was referred for systemic evaluation and treatment.
Excisional Biopsy
Histologic examination revealed multiple fragments of soft tissue with small associated fragments of bone infiltrated in a diffuse pattern by sheets of large atypical lymphoid cells with scant cytoplasm, round to irregular nuclei, vesicular chromatin, and prominent nucleoli (Figures 3 & 4). Mitotic figures are present and apoptotic debris is easily identified (Figure 4). The atypical infiltrate involves skeletal muscle. The atypical cells are positive for CD20, BCL-6, BCL-2 (variable intensity of staining), and MUM-1 (variable, greater than 30% positive) with no convincing expression of CD5, CD10, cyclin D1, CD138, kappa or lambda. Approximately 60% of the atypical cells are Ki-67 positive.
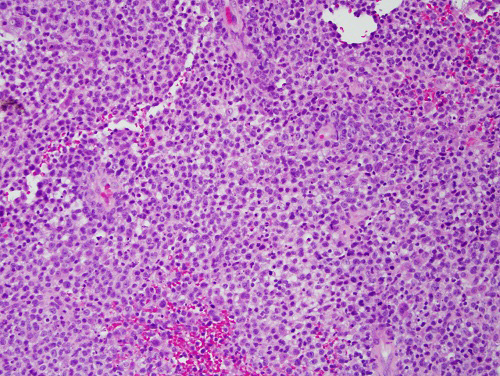
Figure 3. High power (x200) H & E histology shows sheets of large atypical lymphoid cells with scant cytoplasm, round to irregular nuclei, vesicular chromatin, and prominent nucleoli. The atypcial cells infiltrated the nearby skeletal muscle bundles (not shown).
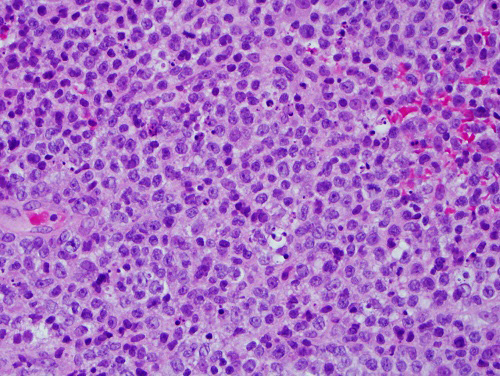
Figure 4. Higher power (x400) H & E histology with closer look at the sheets of large atypical lymphoid cells with scant cytoplasm, round to irregular nuclei, vesicular chromatin, prominent nucleoli and mitotic figures.
After you have finished reviewing the available diagnostic information