Mixed radiolucent radiopaque lesion
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by: Dr. Nadeem Esmail
Eastside Oral Surgery, Bellevue, WA
Case Summary and Diagnostic Information
This is a 5-year-old white male who presents with a large radiolucent and radiopaque lesion associated with an impacted tooth #22.
Diagnostic Information Available
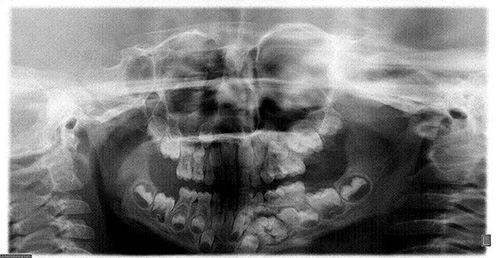
This is a 5-year-old white male who first presented for an initial routine dental examination by the pediatric dentist. Radiographs revealed a large radiopaque and radiolucent lesion associated with an impacted tooth #22 (Figure 1). The lesion was described to be approximately 2 cm in size and was expansile. The lesion displaced tooth #22 into the inferior border of the mandible. The lesion was otherwise asymptomatic; there was no pain or paresthesia. Clinical examination of the area showed an expansion at the left mandibular area overlying the lesion. The overlying and surrounding oral mucosa was unremarkable.
Figure 1. This is a panoramic view of the primary tumor taken at the initial presentation by the pediatric dentist. Note the inferiorly placed and impacted tooth #22 with miniature tooth like structures associated with the crown of the tooth.
The patient’s medical history is unremarkable.
This lesion was discovered during routine oral examination by the patient’s pediatric dentist and was of unknown duration. It was expansile but otherwise asymptomatic. The patient was referred to the oral and maxillofacial surgeon for further evaluation and work up. A panoramic radiograph revealed a large mixed radiolucent/radiopaque lesion in the left mandible (Figure 1). A cone-beam CT scan was also performed to characterize the lesion as well as assess the surrounding structures and amount of surrounding bone present appropriate for the surgical procedure.
Figure 1. This is a panoramic view of the primary tumor taken at the initial presentation by the pediatric dentist. Note the inferiorly placed and impacted tooth #22 with miniature tooth like structures associated with the crown of the tooth.
Treatment
The decision was made to perform an excisional biopsy of the mass under intravenous general anesthesia. A sulcular incision was used to elevate a full thickness mucoperiosteal flap. The thin cortical buccal bone covering the lesion was removed while carefully preserving the surrounding teeth and the inferior alveolar neurovascular bundle. The lesion consisted of many small tooth-like structures with a surrounding sac. The entire lesion was removed without violating the integrity of the mandible. The patient tolerated the procedure well and has had an uneventful postoperative course.
Excisional Biopsy
Histologic examination reveals multiple pieces of decalcified hard and soft tissue embedded in two separate blocks labeled A1 and A2. All specimens are composed of miniature tooth-like structures (Figures 2 & 3) made up of dentin, enamel matrix (Figure 4), and dental pulp (Figures 2 & 3). The tooth-like structures are focally lined by a dental follicle (Figure 2) which is made up of a lining epithelium supported by a fibrous connective tissue wall.
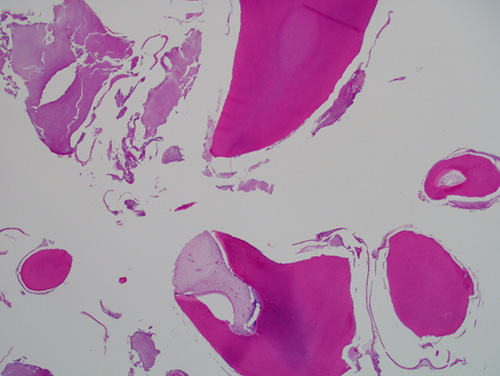
Figure 2. Low power (x40) H & E histology shows multiple tooth-like structures made up of dentin, enamel matrix, pulp and dental follicle focally surrounded by dental follicle lined by epithelium.
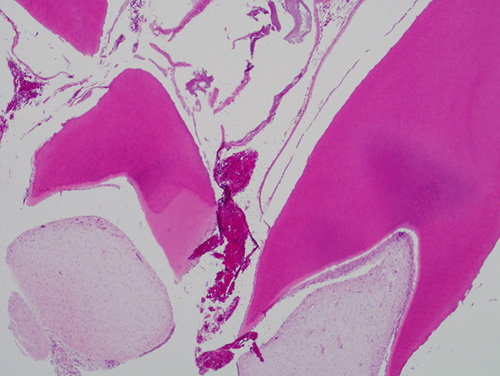
Figure 3. Higher power (x200) H & E histology shows two tooth-like structures with dentin and dental pulp. The dental pulp is superiorly lined by one layer of viable odontoblasts.
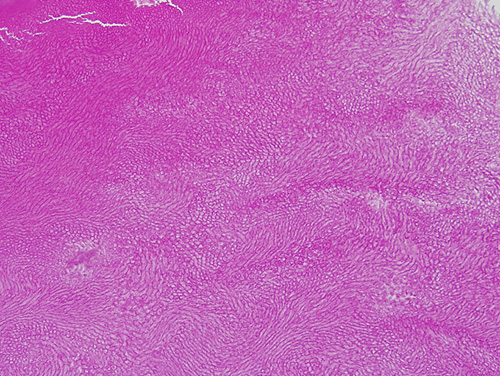
Figure 4. High power (x400) H & E histology shows the enamel matrix at high magnification with the fish-scale appearance.
After you have finished reviewing the available diagnostic information