Return to Case of the Month Archives
Large and multilocular expansile radiolucency, right posterior mandible
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Drs. Ross Beirne, Todd Carter, Ryan Gibson
University of Washington, Seattle, WA
Case Summary and Diagnostic Information

This is a 46-year-old black female who was referred for evaluation of a right posterior mandibular mass of unknown duration. A panoramic radiograph and CT scan revealed a large, impressively expansile, multilocular radiolucency involving the body of the mandible (Figures 1 & 2). The patient reported mild pain in the right side of the mandible. She also reported a feeling of swelling intra-orally.
<h3
This is a 46-year-old black female who was referred for evaluation of a right posterior mandibular mass of unknown duration. A panoramic radiograph and CT scan revealed a large, impressively expansile, multilocular radiolucency involving the body of the mandible (Figures 1 & 2). The patient reported mild pain in the right side of the mandible. She also reported a feeling of swelling intra-orally.
Figure 1 This is a panoramic radiograph demonstrating a large, well-demarcated, multilocular and expansile radiolucent lesion of the right posterior mandible.
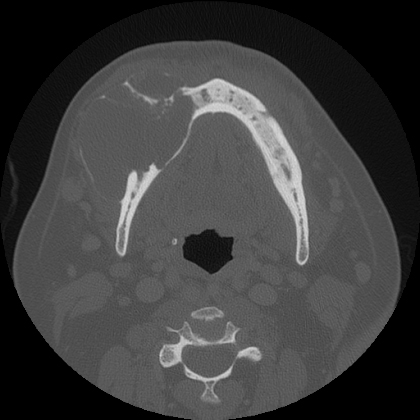
Figure 2 This is a CT scan further demonstrating the expansile nature of this well-demarcated and multilocular radiolucent lesion of the right posterior mandible.
Her past medical history is significant for hypertension, alcoholism and obesity.
Clinical examination demonstrated a large intra-oral (Figure 3) and external swelling of the right body of the mandible. There was evidence of generalized severe periodontitis and multiple missing teeth. Panoramic and CT scan demonstrated a large, multilocular, and well-demarcated radiolucency involving most of the body of the mandible and pushing downward below the inferior border of the mandible (Figure 1). The edentulous anterior labial alveolar ridge also shows evidence of clusters of small soft tissue nodules consistent with inflammatory papillary denture hyperplasia.
Figure 1 This is a panoramic radiograph demonstrating a large, well-demarcated, multilocular and expansile radiolucent lesion of the right posterior mandible.

Figure 3 This is a clinical view of the lesion at presentation demonstrating obliteration of the right mandibular vestibule indicating an expansile swelling in the right mandible. Also, note the inflammatory papillary hyperplasia on the edentulous alveolar ridge overlying the swelling.
Treatment
The procedure was performed under general anesthesia. The tumor was removed through segmental resection of the body of the mandible including the inferior border of the mandible. The surgical specimen was radiographed intraoperatively to reveal the bony margins, which were clear both anteriorly and posteriorly. The surgical site was thoroughly irrigated with bacitracin irrigation and hemostasis was accomplished. A prefabricated 2.7 KLS Martin reconstruction plate was adapted to the right ascending ramus and anterior mandible (Figure 4). The area healed within 4-6 weeks and the overlying mucosa looked pink and healthy. In addition, the patient’s remaining dentition was extracted.
Incisional and excisional biopsy
Histologic examination revealed a solid and benign neoplasm of odontogenic epithelial origin made up of combined epithelial islands and epithelial cords. The islands and cords are surrounded by cellular fibrous connective tissue and are lined by columnar or cuboidal and palisaded epithelial cells (Figure 5). The center of some of the epithelial islands is filled with cuboidal and stellate epithelial cells in most parts and keratin including keratin pearls (Figure 6) in focal areas.
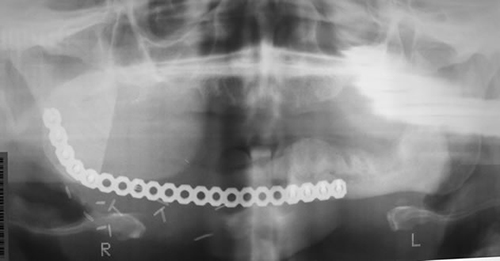
Figure 4 This is a panoramic radiograph represents the post-operative changes consistent with resection of the tumor and replacement with a metal plate adapted to the right ascending ramus and the symphyseal-perisymphyseal region.
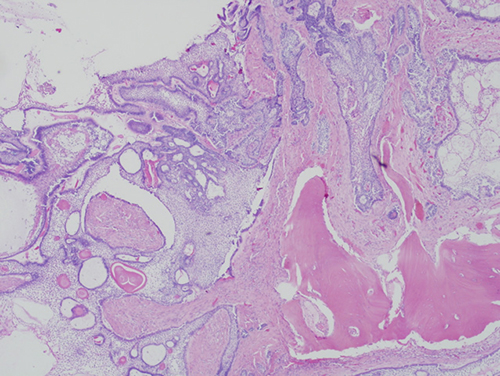
Figure 5 Low power (x100) histology illustrates a benign neoplasm of odontogenic epithelial origin made up of islands and cords of epithelial cells suspended on mature connective tissue. The epithelial islands are lined by one layer of palisaded and polarized columnar cells with areas of reverse polarization. The center of the islands is filled with stellate epithelial cells and keratin, including a few keratin peals.
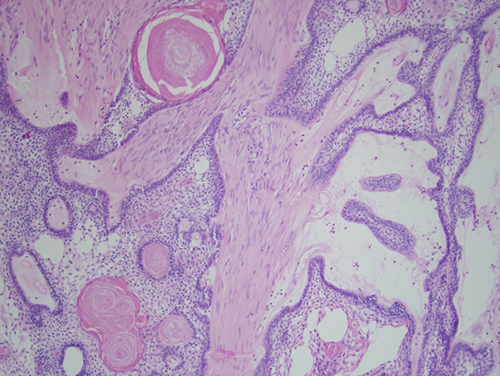
Figure 6 Higher power (x200) histology illustrates a closed look of the epithelial islands with palisaded and columnar periphery and center filled with stellate epithelial cells and keratin.
After you have finished reviewing the available diagnostic information