Return to Case of the Month Archives
Lobulated, fungating, red-blue lesion on the left posterior maxillary alveolar ridge
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Jay Hong
Everett Oral Surgery, WA
Case Summary and Diagnostic Information

This is a 58-year-old white male presenting with a slow-growing lobular, exophytic, red-blue fungating lesion on the left posterior maxillary alveolar ridge.
Diagnostic Information Available
This is a 58-year-old white male presenting with a slow-growing lobular, exophytic, red-blue fungating lesion on the left posterior maxillary alveolar ridge. It is four to five cm in diameter and has been present for one to two months. The lesion is not painful.
Fig. 1 Clinical photograph at presentation, left posterior maxillary edentulous alveolar ridge demonstrates a large, exophytic, lobulated, fungating red-blue exophytic mass
The patient’s past medical history includes a bilateral lung transplant performed in April 1997, secondary to alpha-1 antitrypsin deficiency, and subsequent chronic obstructive pulmonary disease 2. He was recently treated for renal cell carcinoma and end-stage renal disease with radical nephrectomy. Three years ago, a basal cell carcinoma was removed from his left helix using Mohs procedure. He also suffers from hypertension. He is currently taking prednisone, Azathioprine, Sirolimus, Zoloft, Norvasc, Lasix, Lipitor, and Trazadone. PCN and Levoquin.
Histologically, the specimen was made up of a dense, diffuse infiltrate of B-lymphocytes with plasmacytoid differentiation. There was evidence of high mitotic activity and focal necrosis. The Immunohistochemistry studies confirmed that the cells were monoclonal for lambda light chain, uniformly positive for CD138, negative for CD20 and CD45 and strongly positive (70% of the infiltrate) for Epstein-Barr virus. The H & E histology and the immunocytochemistry findings are consistent with a post transplant lymphoproliferative disorder, “plasmacytoma-like” type by the WHO classification system.
Histologically, the specimen was made up of a dense, diffuse infiltrate of B-lymphocytes with plasmacytoid differentiation. There was evidence of high mitotic activity and focal necrosis. The Immunohistochemistry studies confirmed that the cells were monoclonal for lambda light chain, uniformly positive for CD138, negative for CD20 and CD45 and strongly positive (70% of the infiltrate) for Epstein-Barr virus. The H & E histology and the immunocytochemistry findings are consistent with a post transplant lymphoproliferative disorder, “plasmacytoma-like” type by the WHO classification system.
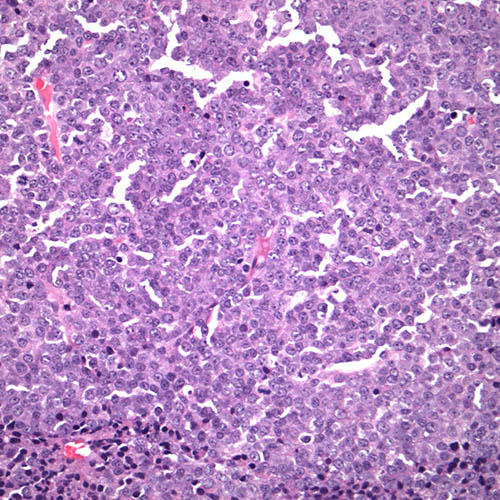
Figure 2. Low power (x100) This represents the H & E histology which shows sheets of monoclonal B-lymphocytes with plasma-cell morphology. There is evidence of necrosis and high-mitotic activity. The histology is consistent with post-transplant lymphoproliferative disorder “plasmacytoid-like”.
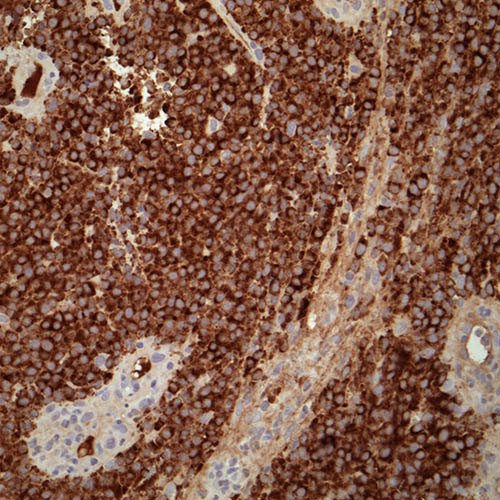
Figure 3. Higher power (x200) This represents the immunohistochemistry staining with antibody to lambda light chain demonstrating uniformly positive tumor cells.
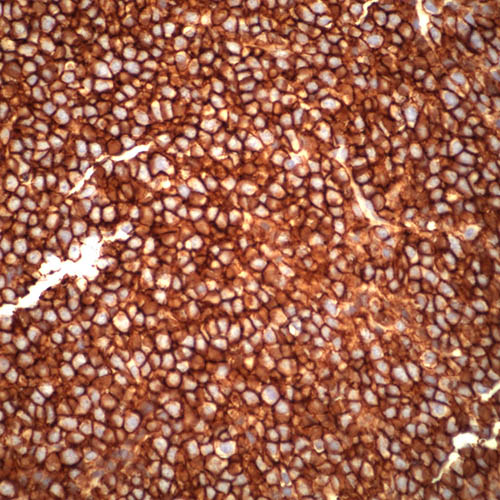
Figure 4. Higher power (x200) This represents the immunohistochemistry staining with antibody to CD138 demonstrating uniformly positive tumor cells.
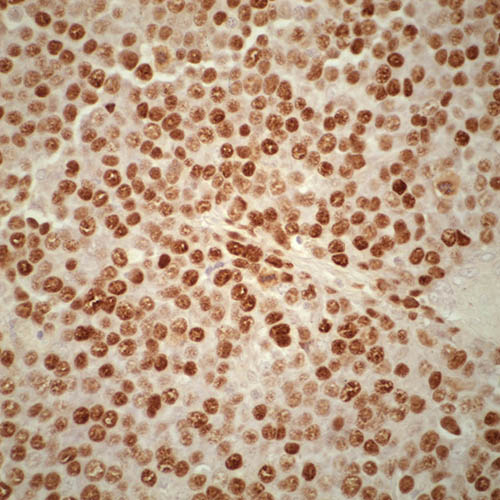
Figure 5. Higher power (x200) This represents the immunohistochemistry staining with antibody to Epstein Barr virus demonstrating uniformly positive tumor cells.
After you have finished reviewing the available diagnostic information