Well demarcated mixed radiolucent/radiopaque lesion between teeth #s 22 & 23
Contributed by Dr. Jared Cottam
Oral & Maxillofacial Surgery, Burien-WA
Case Summary and Diagnostic Information

This is a 53-year-old female who presented with an asymptomatic swelling in the left anterior mandible between teeth #s 22 and 23.
This is a 53-year-old female who presented with an asymptomatic swelling in the left anterior mandible between teeth #s 22 and 23. The involved teeth were vital. The swelling was reported to be slow growing and that it had been present for almost one and a half year. It was approximately 3 X 3 cm in size. It was apical and between teeth spreading the roots apart (Figure 1). Radiographically, the lesion was relatively well-demarcated unilocular and mostly radiolucent with vague cloudy appearance at the periphery of the lesion.
Figure 1 This radiograph is taken at the first clinical presentation. The figure shows a well-demarcated unilocular radiolucency apical and between teeth #s 22 and 23. It is pushing teeth apart and is described clinically as expansile. Note a hint of early and smooth radiopaque look at the periphery of the lesion.
This patient’s past medical history is very limited, social drinker, social smoker 2 cigarettes per week and one glass of wine daily. No major medical issues, patient currently is taking multivitamin.
The patient reports slowly growing swelling in the left anterior mandible (Figure 1) which was otherwise asymptomatic.
Under 2% lidocaine local anesthesia, a vestibular incision was made through the Muco-gingival Junction. Full thickness flap was elevated and corticotomy was done with a bur and copious irrigation. The lesion was curetted and removed. Site was irrigated and sutured closed with 3-0 chromic gut. Patient tolerated the procedure well.
Histologic examination reveals multiple pieces of decalcified hard and soft tissue composed of a benign neoplasm of odontogenic mesenchymal origin. It is made up of connective tissue stroma which is cellular (Figure 2). This neoplasm also contains cementum, most of which is arranged in globules of variable shapes and sizes (Figure 2 & 3). Bone is not identified. The cellular stroma contains remnants of odontogenic epithelium (Figures 2-4), some consistent with “glands of Serres.” The immunohistochemistry with antibody to pancytokeratin highlights the epithelial component (Figure 4).
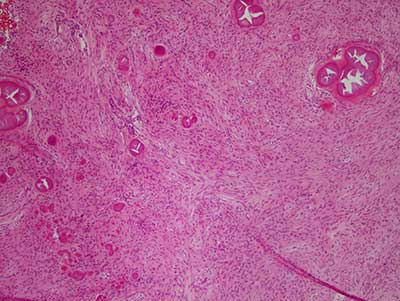
Figure 2 Low power (X100) H & E stained section revealing a cellular odontogenic neoplasm of mesenchymal origin containing globules of cementum-like hard tissue of variable sizes. Also note the nets of epithelial cells scattered throughout the neoplasm
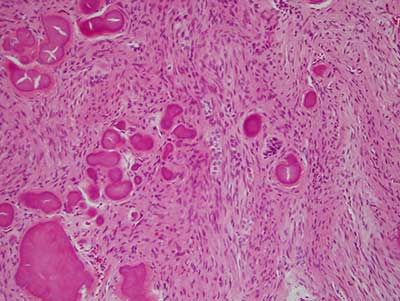
Figure 3 Higher power (X200) H & E stained section revealing a closer look at the neoplasm with connective tissue background and a closer look at the cementum-like globules and the epithelial nests.
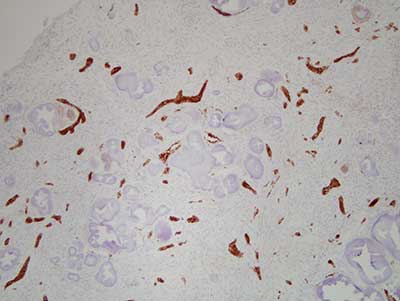
Figure 4 Low power (X100) Immunohistochemistry stain with antibody to pancytokeratin (AE1/AE3) highlighting the nets of epithelial cells throughout the neoplasm.
After you have finished reviewing the available diagnostic information