Return to Case of the Month Archives
November 2010: Widespread Rough White Lesions of Left Mouth
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Pamela Nicoara
Periodontics Clinic, Everett, WA
Case Summary and Diagnostic Information

This is a 58-year-old white male who presented to his dentist with a 9-year history of widespread white lesions involving the left buccal mucosa, left mandibular gingiva and left lateral border of tongue.
Diagnostic Information Available
This is a 58-year-old white male who presented to his dentist with a 9-year history of widespread white lesions involving the left buccal mucosa, left mandibular gingiva and left lateral border of tongue (Figures 1-3). The lesions were white, rough, corrugated, diffuse and leathery in consistency. The lesions were otherwise not painful and not ulcerated. The patient’s past medical history is significant for smoking which he quit smoking ten years ago and replaced the habit with Nicorette gum (ten pieces a day for ten years). The left side of his mouth is where the Nicorette gum was held. The dentist instructed the patient to stop holding the Nicorette gum on the left side, which he did for six months, but the white lesions did not show any evidence of regression (Figures 1-3). However he reduced the number of Nicorette use from ten to eight pieces and that small reduction demonstrates improvement (Figure 4).
Figure 1 This clinical photograph was taken at presentation. Note the diffuse white corrugated white lesions of the left buccal mucosa.

Figure 2 This clinical photograph was taken at presentation. Note the diffuse white corrugated white lesions of the left lateral border of tongue.

Figure 3 This clinical photograph was taken at presentation. Note the diffuse white corrugated white lesions of the left mandibular gingiva.

Figure 4 This clinical photograph was taken at eight weeks after decreasing the number of Nicorette gum from ten a day to eight a day. Compare this photograph to Figure 1 and note the difference in the texture of the buccal mucosa; it is smoother in this figure compared to when he was chewing ten pieces of Nicorette gum per day.
The patient’s past medical history is significant for smoking. These lesions were not present when he smoked and did not appear until years after the Nicorette gum use. The family history is negative for any similar lesions.
The left side of the oral cavity was diffusely white and rough (Figures 1-3). It involved the left buccal mucosa and vestibules, left lateral tongue and left mandibular gingiva, all areas where the Nicorette gum was held. The lesions were white and rough to palpation. They were otherwise asymptomatic.
Figure 1 This clinical photograph was taken at presentation. Note the diffuse white corrugated white lesions of the left buccal mucosa.
Figure 2 This clinical photograph was taken at presentation. Note the diffuse white corrugated white lesions of the left lateral border of tongue.
<3mg class="zoooom" src="https://dental.washington.edu/wp-content/media/com/nov10/Figure3.JPG" width="500" height="333" alt="Figure 1" />
Figure 3 This clinical photograph was taken at presentation. Note the diffuse white corrugated white lesions of the left mandibular gingiva.
Treatment
The left lateral border of the tongue mucosa was biopsied under local anesthesia. An elongated piece of about 8 X 4 X 4 mm in greatest dimensions was removed and submitted for microscopic examination. The area healed within a short period of time. Based on the results of the incisional biopsy, the patient was advised to completely stop the use of the Nicorette gum and switch to a cutaneous nicotine patch.
Incisional Biopsy
Histologic examination reveals a hemisected piece of soft tissue composed of keratinized surface epithelium with underlying fibrous connective tissue (Figure 5). The surface epithelium is covered by a thick layer of parakeratin which is superficially infiltrated by bacterial colonies (Figures 5 & 6). The spinous layer is of increased thickness and shows evidence of reactive atypia in the form of cells with large nuclei and prominent nucleoli (Figure 6). The connective tissue is infiltrated by a few lymphocytes, plasma cells & occasional neutrophils.
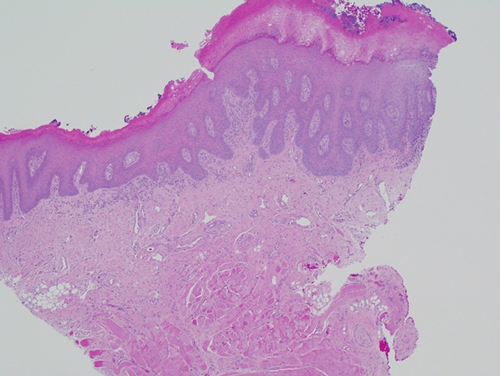
Figure 5 Low power (x40) H & E histology shows a fragment of oral mucosa with a thick keratin layer covered by bacterial colonies. The spinous layer is of increased thickness. The connective tissue is infiltrated by lymphocytes and plasma cells.
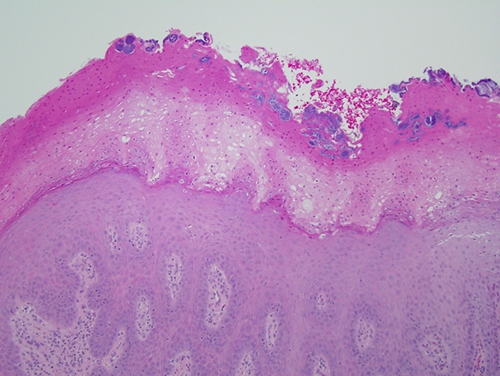
Figure 6 Higher power (x100) H & E histology of the surface epithelium and keratin layer with bacterial colonies.
After you have finished reviewing the available diagnostic information