Return to Case of the Month Archives
Large mixed radiolucent radiopaque lesion,
area of impacted tooth # 32
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Jae Hong
Marysville Oral & Maxillofacial Surgery, Washington
Case Summary and Diagnostic Information

This is a 29-year-old white male referred by his general dentist for a swelling distal to tooth # 32. It was of unknown duration and the patient reported pain in the area. The size of the lesion was about 4 cm at its greatest dimensions. Panoramic radiograph showed a well-demarcated lesion of mixed bony origin with a radiopaque mass in the center and a prominent radiolucent rim at the periphery (Figure 1). Although closely associated, this lesion was clinically separate from the impacted tooth #32.
Diagnostic Information Available
This is a 29-year-old white male referred by his general dentist for a swelling distal to tooth # 32. It was of unknown duration and the patient reported pain in the area. The size of the lesion was about 4 cm at its greatest dimensions. Panoramic radiograph showed a well-demarcated lesion of mixed bony origin with a radiopaque mass in the center and a prominent radiolucent rim at the periphery (Figure 1). Although closely associated, this lesion was clinically separate from the impacted tooth #32.
Figure 1 Panoramic view at first presentation demonstrating impacted tooth #32 associated with a well-demarcated radiolucent/radiopaque mass giving the impressing of pushing tooth #32 inferiorly.
The past medical history is non contributory.
Clinically, a large swelling was identified in the area of tooth # 32. The patient reported pain in the area. Panoramic radiograph showed a well-demarcated lesion of mixed bony origin with a radiopaque mass in the center and a prominent radiolucent rim at the periphery (Figure 1). Radiographically, this lesion appeared to be closely associated with tooth #32. However, at surgery, it was clearly separate from the impacted tooth.
Figure 1 Panoramic view at first presentation demonstrating impacted tooth #32 associated with a well-demarcated radiolucent/radiopaque mass giving the impressing of pushing tooth #32 inferiorly.
Treatment
Under IV sedation, the area was surgically exposed, the lesion was curetted (Figure 2) and tooth # 32 was extracted. The area healed without any complications
Incisional and excisional biopsy
The biopsy specimen was large and was decalcified prior to embedding. It was embedded in three separate blocks and all demonstrated a bone forming neoplasm of osteoblast origin. The neoplasm is made up of bony trabeculae with viable and plump osteocytes occupying large lacunae (Figure 3). The bony trabeculae are surrounded by young osteoblasts and a significant number of osteoclasts (Figure 4). The connective tissue stroma supporting the mineralized bone is loose and vascular.

Figure 2 This photograph is taken during surgery partially exposing the encapsulated lesion.
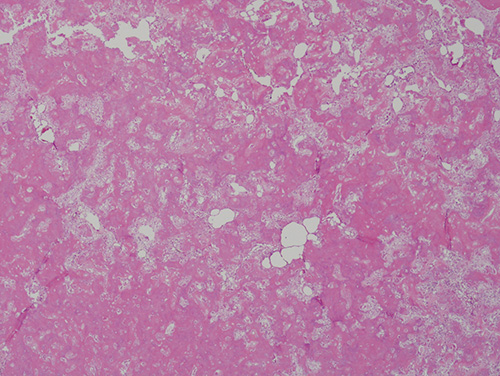
Figure 3 Low power (x100) histology shows a neoplasm of bone origin with cancellous bone surrounded by young osteoblasts and osteoclasts and supported by vascular connective tissue stroma.
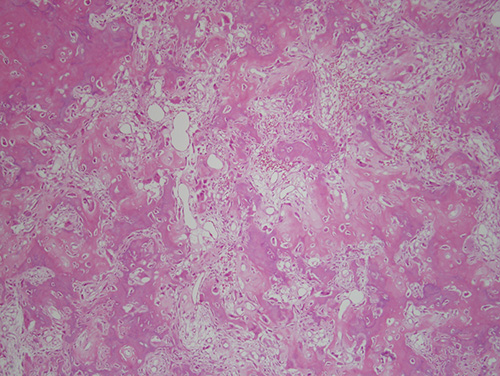
Figure 4 High power (x200) histology shows cancellous bone with young osteocytes occupying large lacunae. The bony trabeculae are surrounded by active osteoblasts and osteoclasts and are supported by vascular connective tissue stroma.
After you have finished reviewing the available diagnostic information