Return to Case of the Month Archives
Diffuse, thick and yellowish-white palate
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. William Paulin
Silverdale Oral & Maxillofacial Surgery
Case Summary and Diagnostic Information

This is a 65-year-old Filipino female with 40+ year history of “reverse smoking”. Reverse smoking is smoking with the lighted end of the cigarette held inside the mouth. She denies alcohol use. She was referred by her general dentist for the evaluation of a diffuse, thick, yellowish-white slightly nodular mucosa of the hard palate, some of which overlying the torus palatinus (Figure 1).
Diagnostic Information Available
This is a 65-year-old Filipino female with 40+ year history of “reverse smoking”. Reverse smoking is smoking with the lighted end of the cigarette held inside the mouth. She denies alcohol use. She was referred by her general dentist for the evaluation of a diffuse, thick, yellowish-white slightly nodular mucosa of the hard palate, some of which overlying the torus palatinus (Figure 1). The patient deferred the suggested incisional biopsy for about six months during which time she essentially discontinued her smoking habit. This resulted in mucosal healing except for two or so small white plaques on her palatal torus (Figure 2). They were completely excised.
Figure 1. This photograph was taken in February 2007. Note the thick and diffuse, white to yellow plaques on the middle and anterior hard palate, some overlying the torus palatinus.
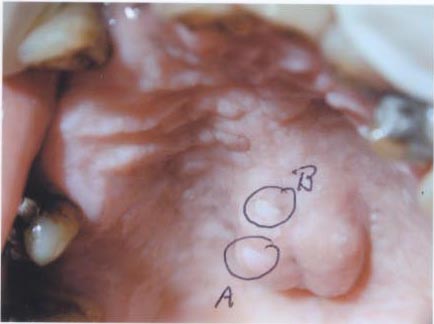
Figure 2. This photograph was taken in August 2007 after six months of cessation of reverse smoking. Note only two small flat white plaques are present overlying the torus palatinus.
The past medical history is significant for 40+ year history of smoking; otherwise the patient is healthy.
In February 2007 (Figure 1), the patient presented with diffuse thick white to yellow plaques on the anterior and middle hard palate. Some of the thick plaques were present over her prominent torus palatinus (Figure 1). The middle hard palate and the maxillary alveolar ridge showed multiple brown macules (figures 1 & 2) which are interpreted to be consistent with smoker’s melanosis but can also be combined racial pigmentation and smoker’s melanosis. There was no evidence of ulceration or erythematous changes. On her second visit (August 2007, after six months of tobacco cessation), most of the thick plaques had disappeared and only two small oval to round thin white plaques were present over the torus palatinus (Figure 2). The two plaques were completely excised and submitted for microscopic evaluation.
Figure 1. This photograph was taken in February 2007. Note the thick and diffuse, white to yellow plaques on the middle and anterior hard palate, some overlying the torus palatinus
<p.Figure 2. This photograph was taken in August 2007 after six months of cessation of reverse smoking. Note only two small flat white plaques are present overlying the torus palatinus.
The histology of both specimens was similar in that the epithelium showed evidence of hyperorthokeratosis (Figure 3) with melanin incontinence (Figure 4) and connective tissue fibrosis consistent with smoker’s keratosis. One of the fragments had verrucoid hyperorthokeratosis. The epithelium was well differentiated and showed no evidence of frank dysplasia.
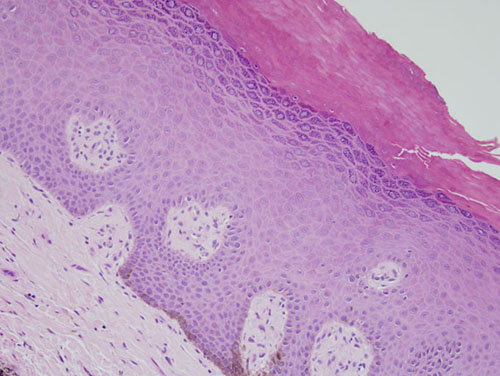
Figure 3. Low power (x100) histology shows a piece of oral mucosa with a thick orthokeratin layer and focal areas of acanthosis and connective tissue fibrosis with basal cell melanosis.
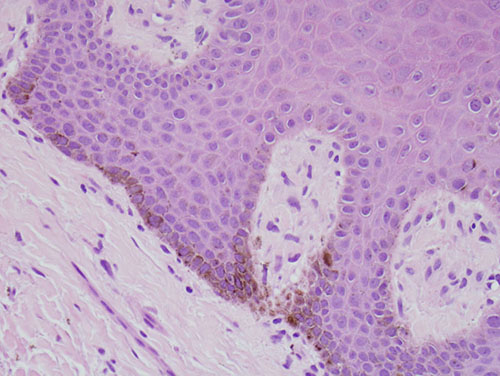
Figure 4. High power (x200) histology shows a piece of oral mucosa with the basal cell layer actively producing and releasing melanin. There is evidence of mild acanthosis and connective tissue fibrosis
After you have finished reviewing the available diagnostic information