Return to Case of the Month Archives
Non-healing ulcer, lateral border of tongue
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Drs. Brian Jackson, Neal Futran
Olympia Oral Surgery and University of Washington
Case Summary and Diagnostic Information

This is a 20-year-old female who was in good health until approximately April 2005 when she noticed a sore on her right lateral tongue.
Diagnostic Information Available
This is a 20-year-old female who was in good health until approximately April 2005 when she noticed a sore on her right lateral tongue (Fig 1). She states that for the past few years she has had recurrent canker sores in this area and thought that this was just another canker sore. However, the pain persisted and by June 2005 she noticed that the lesion had increased in size to a quarter-sized red lesion on the right lateral tongue. She denies any history of bleeding, tongue mobility problems, speech difficulty, dysphagia, odynophagia, or any other symptoms associated with the lesion. The patient presented to an Oral Surgeon who performed an incisional biopsy on 06/14/2005 and sent it for microscopic evaluation; she was then referred to Dr. Futran at the University of Washington Medical Center for further treatment. The patient smokes 2 packs of cigarettes per year and consumes 5 alcoholic beverages per week.

Figure 1. This is a clinical photograph representing the lesion before the incisional biopsy. Single and large, non-healing ulcer on the mid to posterior lateral border of the tongue.
Significant aspects of her medical history include asthma and a right wrist cyst which was excised four years ago. Five years ago, the patient’s mother had parotidectomy for a malignant salivary gland neoplasm that was treated with surgery alone. There is no other family history of head and neck cancer.
She was seen in consultation at the University of Washington Medical Center by Dr. Futran in June 2005. She was found to have a rough, raised lesion involving the right lateral and anterior two-thirds of the tongue. The tumor was superficial in the anterior region while deep in the posterior region. She had a chest x-ray on 06/21/2005, which was negative for any abnormalities. Her CT scan revealed a lymph nodes greater than 1 cm in size.
Histologic examination revealed surface epithelial cells exhibiting changes and invading (Fig 4) the connective tissue, muscle, nerve and one lymphatic space in the form of cords, islands and clusters of cells. The epithelial cells are large with hyperchromatic nuclei and prominent nucleoli, and show high mitotic activity (Fig 5). The epithelial cells are also producing and releasing keratin in the form of individual cell keratinization and keratin pearls (Fig 4). However, the latter is not prominent. These changes are present in both the incisional biopsy specimen and the surgical specimen. All the excised lymph nodes are negative for the presence of neoplastic cells.
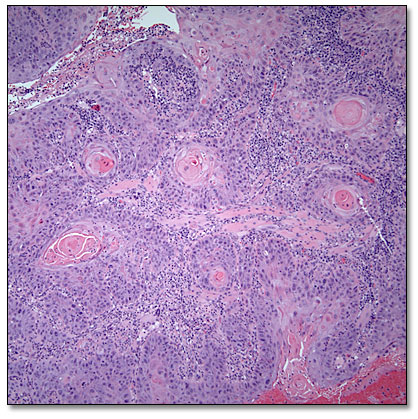
Figure 4. H & E stained section at 100X magnification demonstrating neoplastic epithelial cells of variable sizes invading the connective tissue with keratin pearls.
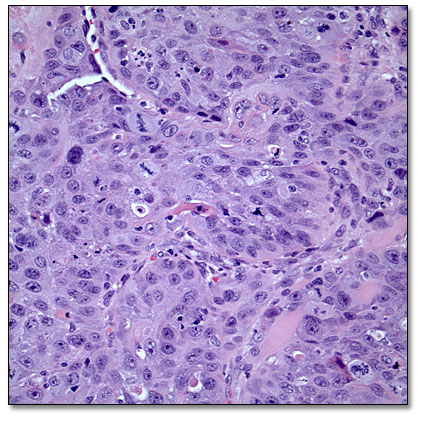
Figure 5. H & E stained section at 200x magnification demonstrating sheets of neoplastic epithelial exhibiting moderate nuclear and cellular pleomorphism and large cells with hyperchromatic nuclei and prominent nucleoli.
After you have finished reviewing the available diagnostic information