Return to Case of the Month Archives
Red, slightly raised nodule, dorsal surface of tongue.
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Brian Jackson, Olympia Oral Surgery
Case Summary and Diagnostic Information

This is an 18-year-old male who was referred to Dr. Jackson for the extraction of his third molar teeth. He was seen initially on December 19, 2005, when he complained of soreness to his third molars. Extra-oral examination was unremarkable. Intra-oral examination revealed no signs or symptoms of an acute infection, but revealed a lesion of unknown duration on the mid-dorsal tongue.
Diagnostic Information Available
This is an 18-year-old male who was referred to Dr. Jackson for the extraction of his third molar teeth. He was seen initially on December 19, 2005, when he complained of soreness to his third molars. Extra-oral examination was unremarkable. Intra-oral examination revealed no signs or symptoms of an acute infection, but revealed a lesion of unknown duration on the mid-dorsal tongue. This lesion was firm, red in color, measured 3-4 mm with no inflammation, and appeared to be devoid of surface filiform papillae (Fig 1). The lesion was otherwise asymptomatic. The patient denied any tobacco and alcohol use. An excisional biopsy was performed on December 20, 2005 and was submitted for histologic evaluation.
His past medical history is negative for medications and allergies. He is a non-smoker, and overall is a healthy individual. In 2000, he had surgery for an open reduction and internal fixation of a wrist fracture, as well as a fixation removal later on.
The intra-oral examination revealed a slightly raised lesion on the mid-dorsal surface of the tongue present amid a fully white tongue. The white color was most likely a result of not brushing the tongue, therefore allowing the accumulation of bacterial colonies on the filiform papillae. The lesion was pink to red in color, firm to palpation, and measured 3-4 mm at its greatest dimensions. The red color was due to a lack of filiform papillae (Fig 1). The lesion was not painful.
Figure 1. This represents the clinical photograph at presentation. Note the white tongue with a red lesion. The white tongue is most likely due to elongated filiform papillae covered with bacterial colonies due to lack of brushing of the tongue. The red color of the lesion is due to filiform atrophy in the area. It is slightly raised because of the underlying osseous choristoma.
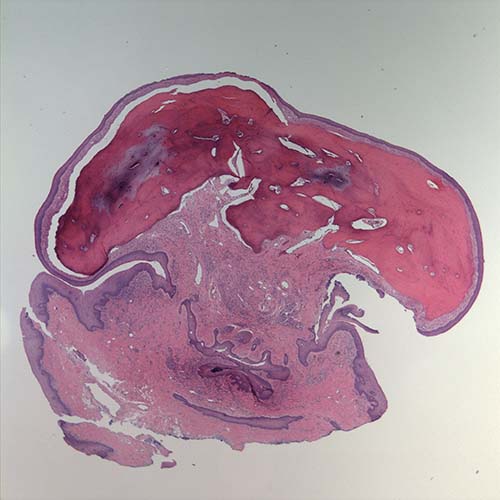
Figure 2. H & E stained section at 20X magnification (low scanning) demonstrating a mass of lamellar bone covered by a thin mucosa. The surface epithelium is stretched and lacks filiform papillae.
The histologic examination revealed a piece of decalcified hard and soft tissue (Fig 2). The latter represented the overlying mucosa with surface epithelium and supporting connective tissue. The bulk of the specimen was made up of an underlying mass of bone (Fig 3) with small spaces containing loose and vascular connective tissue (Fig 4). The bone was lamellar in type with Haversian systems (Fig 4) with viable osteocytes and reversal lines.
Figure 2. H & E stained section at 20X magnification (low scanning) demonstrating a mass of lamellar bone covered by a thin mucosa. The surface epithelium is stretched and lacks filiform papillae.
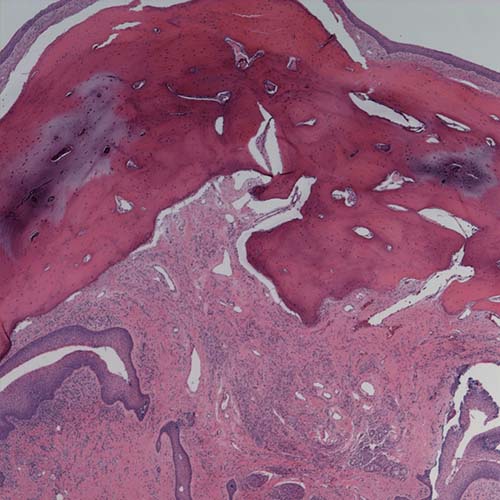
Figure 3. H & E stained section at 100X magnification (low power) demonstrating a mass of lamellar bone covered by a thin mucosa with stretched surface epithelium.
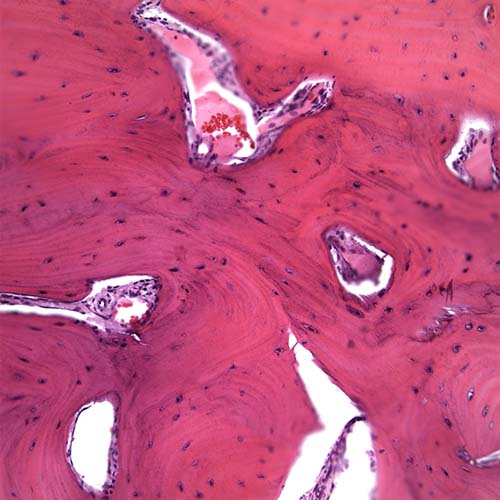
Figure 4. H & E stained section at 400X magnification (high power) demonstrating a mass of lamellar bone with Haversian systems containing viable osteocytes and small spaces with loose and vascular connective tissue.
After you have finished reviewing the available diagnostic information