All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Large multilocular, expansile radiolucency, anterior mandible
Contributed by: Dr. Patricia Kelly
University Oral & Maxillofacial Surgery, Seattle, WA
Case Summary and Diagnostic Information
This is a 30-year-old female presented to her dentist, as a new patient, with an expansile swelling in the anterior mandible.

This is a 30-year-old female presented to her dentist, as a new patient, with an expansile swelling in the anterior mandible. A panoramic radiograph was taken which demonstrated a large multilocular lesion (Figure 1). The lesion is of unknown duration and the patient was unaware of the lesion until it was pointed out to her. She denies any sensory disturbances; she denies pain.
Figure 1 This panoramic radiograph was taken at first clinical presentation. Note the large multilocular radiolucency with well-demarcated margin between teeth #s 19-29. Areas of expansion and extreme thinning of the facial cortical bone noted in the anterior mandible.
The patient’s past medical history is significant for Asthma, GERD, IBS, Generalized anxiety disorder and dental phobia.
Clinically, there is a firm expansile and depressible blue-colored swelling of the anterior mandibular vestibule (Figure 2). The panoramic radiograph revealed a large and well-demarcated multilocular radiolucency in anterior mandible extending bilateral posterior mandible (Figure 1). The CBCT images supported the panoramic radiograph findings. The lesion was expanding the anterior facial plate of the mandible and causing significant thinning of the cortex (Figure 1). There are no signs of root resorption.
After ten months, follow up radiographs (Figure 3) show signs of likely residual lesion, but recurrence cannot be definitively excluded. There are signs of bony healing, and persistent radiolucent lesion mostly at the left mandible. The anterior mandible is not completely filled in with bone and there are signs of loss of facial cortex. The right mandible appears to show normal bone healing.

Figure 2 This photograph was taken at first clinical presentation. Note the large grayish-purplish swelling in the anterior mandibular vestibule reflecting through the mucosa.
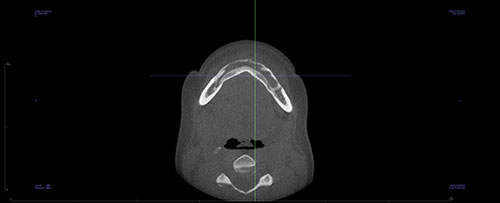
Figure 3 This CBCT is taken after ten months post excisional surgical removal of the lesion shown in Figure 1. There is clear evidence of mildly expansile radiolucency in the left anterior mandible.
The patient had three separate surgical interventions of the area.
1. The first procedure represented an incisional biopsy for histopathologic diagnosis, performed under IV sedation.
2. Prior to excisional biopsy of the entire lesion, multiple teeth were root canal treated in anticipation of loss of blood supply to these teeth and pulp necrosis (teeth #s 21 through 29). The second procedure represented excisional removal and curettage of the lesion under intubated general anesthesia. The surgical site showed multiple areas of cortical bone perforation. The anterior mandible facial plate was severely thinned (Figure 4).
3. Approximately one year post excisional surgical removal of the lesion, residual lesion (or perhaps recurrent lesion) was once again curetted under intubated general anesthesia and the curetting were submitted for microscopic examination.

Figure 4 This photograph was taken during the excisional surgical removal of the lesion. Noted loss of bone around roots and perforation through the facial cortex.
Histologic examination reveals multiple pieces of soft tissue composed of loose and myxoid connective tissue (Figure 5). It is made-up of stellate and small spindle-shaped fibroblasts suspended on delicate collagen fibers (Figures 6 & 7). In some areas, the myxoid connective tissue is hypocellular while in others it is slightly more cellular and has thicker collagen fibers. There is no evidence of an epithelial component or tumor-produced calcified material. There is evidence of host bone surrounded by the myxoid connective tissue. The immunohistochemistry stain is negative with S100 (not shown) which rules out myxoid peripheral nerve neoplasm.
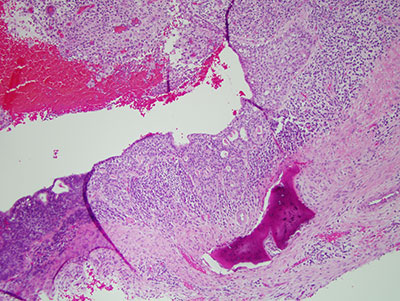
Figure 5 Low power (x40) histology of H & E stained section demonstrating a cystic structure with lining epithelium supported by heavily inflamed fibrous/granulation tissue wall. The lining epithelium contains microcyst-like structures.
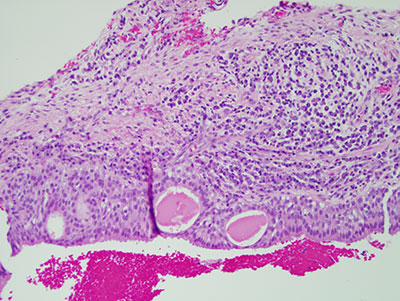
Figure 6 Higher power (x100) histology of H & E stained section shows a closer look at the lining epithelium with microcyst-like structures focally lined by cuboidal cells. Also note the very superficial layer of the lining epithelium covered by one layer of ciliated cuboidal cells.

Figure 7 Higher power (x100) histology H & E stained section shows a closer look at the lining epithelium containing clusters of mucous producing cells.
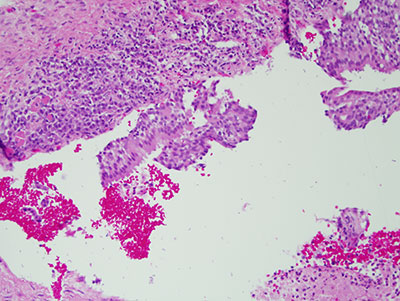
Figure 8 High power (x200) histology of H & E staining section with closer look at the ciliated cuboidal layer of cells covering the top portion of the lining epithelium.
After you have finished reviewing the available diagnostic information