Large multilocular, expansile radiolucency, right posterior mandible
All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Contributed by: Dr. John Malan
Owyhee Oral & Facial Surgery, Nampa Idaho
Case Summary and Diagnostic Information

This is a 20-year-old white male who was referred by his general dentist for a large swelling on the right mandible.
This is a 20-year-old white male who was referred by his general dentist for a large swelling on the right mandible. The patient reports “I think my wisdom tooth is coming in and causing a lot of swelling; it has gotten so bad I can’t put my teeth together.” The patient was seen in 2016 by another general dentist who took a panoramic radiograph noticing displacement of tooth #32 into the ramus (Figure 1). The tooth displacement was interpreted to be related to “eruption of tooth #32.” Due to a rapid increase in swelling over the last 3 months, a new panoramic image was obtained which showed a large, multilocular and expansile radiolucency extending from the apex of tooth #28 to the superior right mandibular ramus, displacing tooth #32 posteriorly and superiorly to the coronoid process (Figure 2).

Figure 1 This first panoramic radiograph was taken in 2016 when tooth #32 was noted to be displaced posteriorly. There is a relatively defined radiolucency between teeth #s 31 and 32.
Figure 2 This panoramic radiograph was taken two years after that displayed in figure 1. Note the destructive and large multilocular and expansile radiolucency between teeth #s 29 and 32. The latter tooth is further pushed posteriorly into the coronoid process.
The patient’s past medical history is unremarkable.
Patient reported severe swelling and mobility of teeth #s 30 and 31 over the last several weeks (Figure 2). The area has been progressively enlarging over the last 3 months.
Under local anesthesia, an incisional biopsy was performed. After the incisional biopsy, the patient was referred for treatment of the remaining lesion.
Histologic examination revealed multiple fragments of soft tissue composed a neoplasm of odontogenic mesenchymal origin. The neoplasm is made up of myxoid and scantly cellular connective tissue made up of small and spindle-shaped cells suspended on delicate collagen fibrils (Figures 3 & 4). In other areas, the connective tissue is more fibrotic with short strands of collagen bundles. The immunohistochemistry with antibody to S100 protein is negative (not shown) ruling out a neoplasm of peripheral nerve origin.
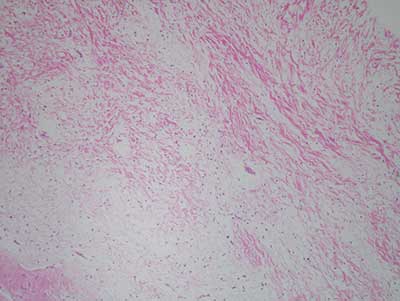
Figure 3 Low power (x100) H & E histology illustrates myxoid fibrous connective tissue stroma made up of a small number of benign stellate and spindle-shaped fibroblasts suspended on delicate collagen fibers, myxoid background and few small blood vessels.
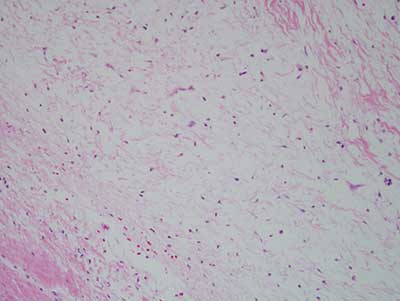
Figure 4 Higher power (x 200) H & E histology illustrates myxoid fibrous connective tissue stroma made up of a small number of benign stellate and spindle-shaped fibroblasts suspended on delicate collagen fibers, myxoid background and few small blood vessels.
After you have finished reviewing the available diagnostic information