Single smooth surfaced and well-demarcated nodule, floor of mouth
Can you make the correct diagnosis?

This is a healthy six-year-old boy with a single asymptomatic, smooth-surfaced, dome-shaped exophytic nodule on the floor of the mouth referred to as “sublingual ranula”.
Sorry! you are incorrect
The location and the clinical description of “doughy consistency” is characteristic of a ranula. The histology, however, is not supportive of a ranula.
Mucoceles and ranulas are clinical terms describing exophytic, fluid filled, fluctuant nodules, typically of minor salivary gland origin and present mostly on the lower lip and the floor of the mouth (1-2). Over 90% of these lesions are cyst-like structures, or pseudocysts, and are mucous extravasation phenomena referred to as mucoceles. Some of these lesions are true cystic structures lined by epithelium and filled with mucus and are called mucus retention cysts or salivary duct cysts. These constitute a small percentage of all mucoceles (1-3). Ranulas, mucoceles of the floor of the mouth, constitute the other 5% and are divided into those above the mylohyoid muscle (majority) and below the mylohyoid muscle (also known as plunging ranulas or cervical ranulas) (3). Ranulas are of minor or major salivary gland origin and are mostly extravasation in type. The etiology of the extravasation mucoceles is usually sharp trauma cutting through the salivary gland duct and releasing the mucous in the extracellular tissue (1-2). Histologically, the extravasation-type mucocele consists of a cyst-like structure lined by granulation tissue and filled with mucoid material, foamy macrophages, and at times small clusters of neutrophils. The mucous retention cysts develop as a result of a duct blockage which can be caused by trauma, fibrosis, sialolith, or pressure from an overlying tumor (1). The extravasation mucoceles most commonly occur on the lower lip and very rarely on upper lip. They may occur anywhere else in the oral cavity, including the buccal mucosa and floor of mouth (Ranula). The latter can be of minor salivary gland or submandibular or sublingual gland duct origin (2-3) and is more commonly seen in children and adolescents. It presents as a swelling with a bluish color if superficial, while deep mucoceles tend to take the color of the surrounding mucosa. Mucoceles tend to fluctuate in size. They are usually associated with a history of sharp lip or cheek biting, but can also be secondary to surgery in the area. This is especially true with the anterior tongue mucoceles. Surgical excision with the associated minor salivary gland is the preferred treatment for the deep mucoceles; superficial mucoceles can self-heal within 2-3 weeks. Superficial mucoceles can also mimic vesiculobullous-type diseases because they look like vesicles (1), especially when presenting in multiples (rare, but described). They can recur if the source of trauma is not eliminated or if they are secondary to surgery. Simple (non-plunging) ranula is best treated by marsupialization into the floor of mouth (1-3). Plunging ranula requires complete excision via an extra-oral approach. The technical difficulties associated with the complete removal of this thin-walled lesion result in a relatively high recurrence rate.
Congratulations! You are correct
Dermoid cysts of the oral cavity are rare and constitute around 1.6% of all Dermoid cysts according to the original 1937 report by New and Erich (6). They are more common in the testis than in any other location, followed by the ovaries and the head and neck area (6-8). In the latter area, the floor of mouth is one of the more common areas of occurrence. This cyst is clinically classified into three types and is based on its relationship to the floor of mouth muscle, the geniohyoid and mylohyoid muscles (7). The more common presentation is above the geniohyoid and mylohyoid muscles, which are clinically visible (as is the case in this patient) in the floor of mouth as they push the tongue upward, leading to dysphagia, dyspnea and dysphonia. If it is between the geniohyoid and the mylohyoid muscle or below the mylohyoid muscle, it would create the appearance of a double chin. The third type is where the cyst displaced laterally into the submandibular area (8). Dermoid cysts of floor of the mouth are rarely described in children under the age of 10. The majority occur between the ages of 10 and 30 for the floor of mouth and 15 and 40 for the ovaries. Dermoid cysts above the geniohyoid muscle present as a slowly enlarging large, round, raised and smooth-surfaced nodules. The nodule is usually painless unless it is infected, when pain can set in. Infected cysts can drain through either an intraoral or extraoral fistulas. The size of the lesion determines its interference with eating, speaking and swallowing. This cyst is classified histologically into two types: cystic structures with a lumen filled with keratin and a connective tissue wall with skin adnexa and true cystic teratomas with all three germ layers tissues such as the brain, bone, muscle, respiratory and gastrointestinal tissues. The oral Dermoid cysts tend to be simple with skin adnexa in the wall. The true teratoma type cysts (more in the ovary) are prone to malignant transformation more so than those in the floor of mouth. Treatment of choice is surgical removal via intra or extra oral approach, depending on where the cyst is located.
Treatment
Under general anesthesia and with a trans-oral approach (Fig 2), an incision was made through the anterior floor of the mouth. The cyst was bluntly and circumferentially enucleated. It shelled out intact as an encapsulated white nodule (Figs 2 & 3) of about 1.5 cm in size. The nodule was soft, and upon sectioning it was filled with white cheesy material consistent with keratin (Fig 4). The surgical site was closed with Vicryl suture around a 1.5cm Penrose drain. The area healed well.

Figure 2. This is a clinical photograph of the lesion at surgery demonstrating a whitish-yellow nodule emerging from the site of incision.
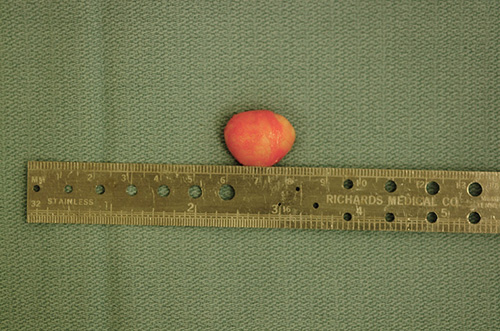
Figure 3. This is a gross photograph of the nodule after it was removed from the floor of mouth. It is whitish-yellow in color.

Figure 4. The nodule in figure 3 is bisected. It shows a sac full of keratin emerging as white cheesy material.
References
- McGurk M. Management of the ranula. J Oral Maxillofac Surg. 2007 Jan;65(1):115-6.
- Chidzonga MM, Mahomva L. Ranula: experience with 83 cases in Zimbabwe. J Oral Maxillofac Surg. 2007 Jan;65(1):79-82.
- Loney WW Jr, Termini S, Sisto J. Plunging ranula formation as a complication of dental implant surgery: a case report. J Oral Maxillofac Surg. 2006 Aug;64(8):1204-8
- Foley DS, Fallat ME. Thyroglossal duct and other congenital midline cervical anomalies. Semin Pediatr Surg. 2006 May;15(2):70-5
Thyroglossal - New, G. B., and Erich, J. B. Dermoid cysts of head and neck. Surg. Gynecol. Obstet. 65: 48, 1937
- Meyer, I. Dermoid cysts (dermoids) of the floor of the mouth. Oral Surg. Oral Med. Oral Pathol. 8: 1149, 1955
- Zachariades, N., and Skoura-Kafoussia, C. A life threatening epidermoid cyst of the floor of the mouth: Report of a case. J. Oral Maxillofac. Surg. 48: 400, 1990
- Clark S, Greenwood M, Fullarton M, Russell JS. An unusual case of floor of mouth swelling: case report, differential diagnosis and a review of the literature. Dent Update. 2005 Dec;32(10):617-9
- Furlong MA. Fanburg-Smith JC, Childers ELB. Lipoma of the oral and maxillofacial region: Site and subclassification of 125 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004 Oct;98(4):441-50
- Fregnani E.R, Pires FR, Falzoni R, Lopes MA and Vargas PA. Lipomas of the oral cavity: clinical findings, histological classification and proliferative activity of 46 cases. Int J Oral Maxillofac Surg 32 (2003), pp. 49–53.
- Fletcher C.D.M. Unni KK and Mertens F. Adipocytic tumors. In: Pathology and genetics: tumours of soft tissue and bone. World Health Organization classification of tumours, IARCPress, Lyon, France (2002), pp. 9–46
Sorry! you are incorrect
The location is unusual for this cyst. The histology is not supportive of this cyst.
Thyroglossal duct cyst is an uncommon cyst. It arises along the embryonal thyroglossal tract, which is between the foramen cecum in the posterior tongue and the thyroid gland. Up to 80% occur below the hyoid bone (4-5). This cyst presents at any age, but is more common in young individuals; 50% occur in patients under 20 years of age. It is usually a firm, cystic mass in the midline. It is of variable sizes. It is usually asymptomatic and slow growing, but dysphagia may occur if it occurs in the higher portion of the tract (4). A fistula may also develop if it gets infected. It has a characteristic histological presentation of a cystic cavity lined by epithelium and supported by a connective tissue wall containing mucous secreting glands, thyroid follicles, benign lymphoid aggregates and others (5). Complete surgical removal is the treatment of choice; however, given the difficulty of removing the tract the lesion may recur and complete removal may be a challenge. The overall prognosis is good. Recurrence depends on the completeness of removal. Squamous cell carcinoma within the lining epithelium has been described.
Sorry! you are incorrect
The clinical description of “doughy consistency” is consistent with a lipoma. Although rare in the mouth, this lesion has been described in the floor of mouth. Lipomas are also rare in children. The histology is not supportive of a lipoma.
Lipomas are benign neoplasms of adipose tissue origin (9-10). They are more commonly described in the trunk and extremities (12) and are rare in the oral cavity. Their overall incidence in the oral cavity is around 4.4% of all benign oral lesions(10). In a recent study from the Armed Forces Institute of Pathology (AFIP) of 125 benign lipomas in and around the mouth, the male to female ratio was approximately 3:1, which is not surprising given the study was extracted from a Military population. Other studies reveal an equal gender distribution (11). The AFIP study showed the mean age to be 52 with a range of 9-92 years (10). Only 4 of the 125 cases involved patients under 18 (10). In the mouth, the most common location for this neoplasm is the buccal mucosa followed by lips, submandibular area, tongue palate and less on the floor of mouth and vestibule (10-11). These findings are consistent with many other published reports. These lesions are slow-growing and can be present for many years. Lipomatous nodule of the buccal mucosa may represent herniation of the buccal fat pad. Lipomas usually present as a single, smooth surfaced, soft with doughy consistency, lobulated, painless, yellowish, sessile nodule (9-11). The overlying mucosa is usually thin and stretched with visible blood vessels. Because of its softness it can be mistaken for a cyst. Histologically, lipomas are variable benign histologies. Some have predominant lobules of mature adipocytes surrounded by a thin connective tissue capsule, while others have predominant spindle-cell component, myxoid, chondroid, connective tissue component. Some are intramuscular (12). Each has its own clinical behavior. Simple surgical excision is the treatment of choice for the simple, mature adipocyte component.