Return to Case of the Month Archives
Swelling of the Lower Anterior Jaw
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Philip Worthington, University of Washington, and Dr. Robert Dixey, Bellevue, WA
Case Summary and Diagnostic Information

This is a 14-year old white male who presented with a swelling of the right symphysis and parasymphysis area.
Diagnostic Information Available
This is a 14-year old white male who presented at the University of Washington Oral Surgery clinic with a swelling of the lower anterior jaw in the right symphysis and parasymphysis area.
The patient’s past medical history includes orthodontic treatment of one-year duration during which time there was little or no movement of teeth. He has had no prior surgery, no allergies, and is not on any medications. There is no family history of related disease.
Clinical examination revealed mild swelling in the anterior and posterior mandible. The radiographic findings were striking (Figures 1, 2).
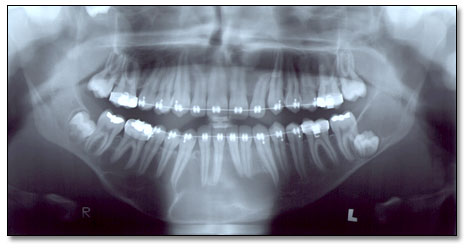
Figure 1. Panoramic view at first presentation demonstrating a total of five cysts, area of teeth #s 1 (impacted), 16 (missing), 9-12, 17 (impacted) and 21-31. The latter cyst is the largest and is multilocular compared to the other four unilocular radiolucencies.
There were a total of five radiolucencies: three in the maxilla and two in the mandible. The three in the maxilla were unilocular radiolucencies around impacted tooth # 1, missing tooth #16 and between teeth #s 9 and 12.
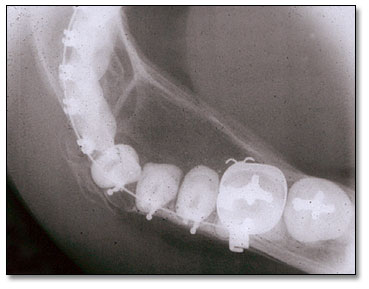
Figure 2. Occlusal view of the large mandibular cyst demonstrating a multilocular radiolucency with buccal and lingual expansion.
The two cysts present in the mandible were a unilocular radiolucency with a scalloped border, associated with tooth # 17 and extending into the ramus; and a large multilocular radiolucency between teeth #s 21 and 31. The large cyst hollowed more than two thirds of the mandible. A sixth cyst developed within the first year of presentation in the area of impacted tooth #32.
Histological examination of all cysts with the exception of the marsupialized cyst were similar in morphology. A cystic structure with uniformly thin, keratinized and corrugated lining epithelium with palisaded basal cell layer and a supporting fibrous connective tissue wall was identified in each specimen. The lumen was filled with keratin (Figure 6). The histology of the cyst in the anterior mandible changed after marsupialization; prior to marsupialization, it was non-keratinized and proliferative stratified squamous epithelium lacking the characteristics of typical OKC morphology.
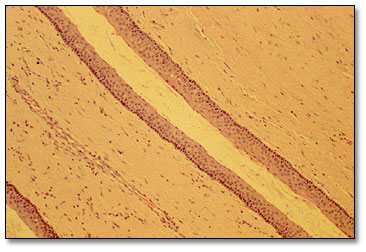
Figure 6. Low power (x100) histology shows a cystic structure with lining epithelium and a supporting fibrous connective tissue wall. The lining epithelium is uniformly thin and is corrugated and keratinized with palisaded basal cell layer
After you have finished reviewing the available diagnostic information