All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Expansile, radiopaque/radiolucent lesion, right posterior mandible
Contributed by: Dr. Craig Neal
Oral & Maxillofacial Surgery, Seattle, WA
Case Summary and Diagnostic Information
The patient is a 67-year-old female who presented with diffuse pain in the right posterior mandible in edentulous area of tooth #29 affecting tooth #29.
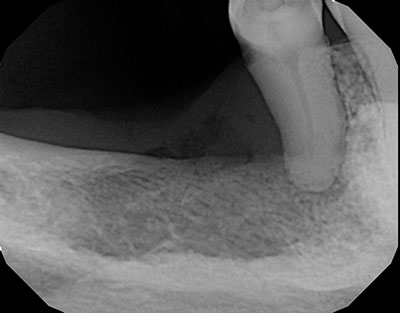
The patient is a 67-year-old female who presented with diffuse pain in the right posterior mandible in edentulous area of tooth #29 affecting tooth #29. Clinically, it looked like a portion of her lingual mandibular torus had collapsed. A periapical x-ray (Figure 1) shows significant bone density loss with orange-peel appearance. Tooth #29 is mobile and tender. The patient is not a current smoker but has previous history of cigarette smoking.
Figure 1 This is a periapical radiograph taken at first visit to the dentist in 2019. The radiographic changes are in the posterior, predominantly radiopaque in area distal to tooth #29. This tooth shows loss of bony support.
The patient’s past medical history is significant for aortic aneurysm, atrial fibrillation and anemia.
The last time this patient saw a dentist was in April 2017 (Figure 2) where a periapical radiograph shows an edentulous area in the right posterior mandible (same site as that of Figure 1) demonstrating normal bony trabeculae and no evidence of resorption. Dating back to 2014 (Figure 3), is a panoramic view of the area demonstrating teeth #s 28 and 29 well supported by normal bone. All three figures show an overlap image of a radiopaque mass consistent with torus mandibularis. The patient was lost for follow-up for nearly two years from 2017 to 2019. Figure 1 is from recent 2019 which shows significant changes in the alveolar bone in area of tooth #29 and distally. The changes are associated with pain. The overlying gingiva/mucosa was erythematous and looked inflamed. Tooth #29 was mobile and tender.
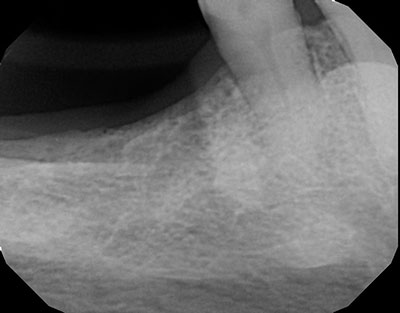
Figure 2 This is a periapical radiograph taken in 2017-last visit to the dentist before that of Figure 1. The periapical radiograph is for the same site to include tooth #29 and distally. As noted, the alveolar bone has normal trabeculae and the tooth has good bony support.

Figure 3 This is a panoramic radiograph taken by the same dentist in 2014. Teeth #s 28 and 29 are present with good bony support and normal alveolar bone surrounding the area.
Incisional biopsy was performed under local anesthesia and IV sedation. An incision was made in the area. Tooth #29 was extracted and small fragments of soft tissue were removed and submitted for histopathologic examination.
Histologic examination reveals multiple pieces of soft tissue composed of mature fibrous connective tissue infiltrated by epithelial islands, cords and nests (Figure 4). The connective tissue was partially lined by oral mucosa exhibiting high-grade atypia focally invading the connective tissue (Figure 5). The neoplastic epithelial islands display very dark (hyperchromatic) nuclei and alteration in the nuclear/cytoplasmic ratio. There was evidence of individual cell keratinization, occasional keratin pearls and mitotic activity.
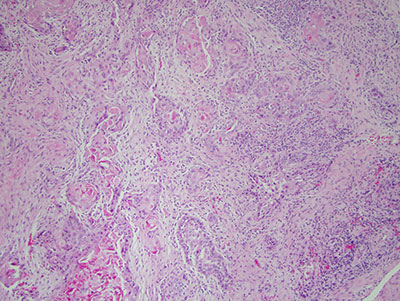
Figure 4 Low power (x40) H & E histology illustrates fragments of soft tissue made up of mature connective tissue infiltrated by many neoplastic epithelial islands, cords and nests. These cells show evidence of nuclear and cellular pleomorphism and nuclear hyperchromatism.

Figure 5 Higher power (x100) H & E histology illustrates fragments of soft tissue made up of mature connective tissue partially covered by surface epithelium exhibiting high-grade epithelial atypia and invading the connective tissue.
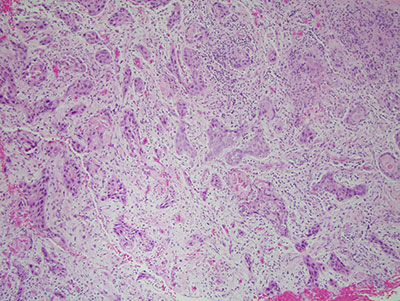
Figure 6 Higher power (x100) H & E histology illustrates fragments of soft tissue made up of mature connective tissue infiltrated by many neoplastic epithelial islands, cords and nests. These cells show evidence of nuclear and cellular pleomorphism and nuclear hyperchromatism, individual cell keratinization and rare keratin pearls.
After you have finished reviewing the available diagnostic information