Large Radiolucency & Corresponding Exophytic Soft Tissue Mass, Right Posterior Mandible
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by: Drs. Clem Pellet and Namou Kim
OMS & ENT Surgery, Bellevue & Seattle, WA
Case Summary and Diagnostic Information

This is a 24-year-old white female who presented with significant pain associated with a large and ulcerated mass in the posterior mandible and the retromolar pad area.
Diagnostic Information Available
This is a 24-year-old white female who presented with significant pain associated with a large and ulcerated mass in the posterior mandible and the retromolar pad area (Figure 1). It was of five days’ duration and was stated to be associated with a traumatic incident related to eating a corn husk. The patient complained of not being able to close her mouth. The panoramic (Figure 2) and CT radiographs demonstrated a mildly expansile and well-demarcated radiolucent lesion in the right posterior mandible extending into the ramus area. There was superior cortical bone dehiscence.
Figure 1. This photograph was taken at first clinical presentation to the oral surgeon complaining of pain and swelling of five-day duration. Note the deeply ulcerated soft tissue swelling in the right retromolar pad area. At this point, the patient was having difficulty closing her mouth.
The patient’s past medical history is significant for a right pharyngeal mass that was removed in 2004 but otherwise is negative for any significant diseases or risk factors.
The patient reported pain and swelling in the right retromolar pad area (Figure 1) of five days’ duration. The lesion developed in response to trauma. The surrounding teeth were vital. Panoramic radiograph (Figure 2) revealed a large radiolucency in the posterior mandible present directly beneath the soft tissue swelling. The bony lesion was mildly expansile but was of unknown duration.
Figure 1. This photograph was taken at first clinical presentation to the oral surgeon complaining of pain and swelling of five-day duration. Note the deeply ulcerated soft tissue swelling in the right retromolar pad area. At this point, the patient was having difficulty closing her mouth.
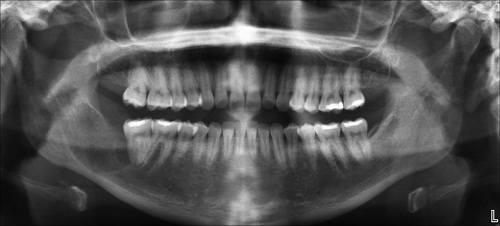
Figure 2. Panoramic radiograph taken at first clinical presentation. Note the large, well-defined radiolucency involving area of tooth #31 and extending posteriorly into the ramus. Also note, it is pushing the inferior alveolar canal but not arising from it.
Treatment
Under local anesthesia, the exophytic soft tissue lesion was biopsies. The specimen was submitted for microscopic evaluation and the diagnosis led to a referral for complete removal of the exophytic soft tissue and the underlying bony lesion.
Excisional Biopsy
Histologic examination reveals a multisected piece of soft tissue made up of a neoplasm of odontogenic mesenchymal origin. This neoplasm is made up of myxoid fibrous connective tissue with spindle-shaped cells that are haphazardly arranged in most parts (Figure 3). The neoplastic cells are suspended on delicate collagen fibers in some areas and more mature and dense collagen in others (Figure 4). This neoplasm is focally infiltrated by a few lymphocytes.
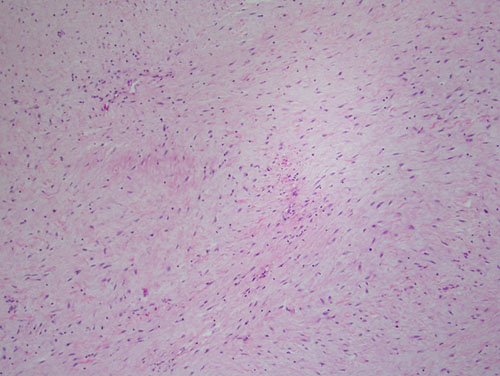
Figure 3. Low power (x100) H & E histology illustrates myxoid fibrous connective tissue with spindle shaped cells suspended on a delicate background of collagen fibers in most parts and more mature and dense collagen bundles in focal areas.
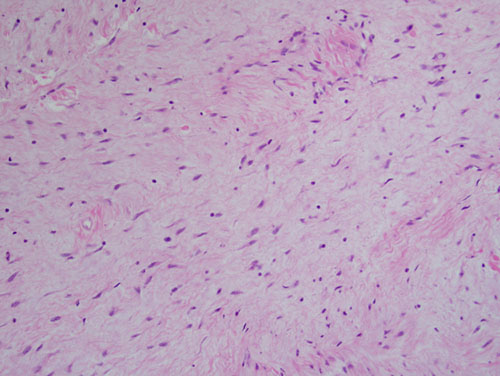
Figure 4. Higher power (x200) H & E histology illustrates myxoid fibrous connective tissue with spindle shaped cells suspended on a delicate background of collagen fibers in most parts and more mature and dense collagen bundles in focal areas.
After you have finished reviewing the available diagnostic information