June 2010: Large radiolucency with scalloped border, right posterior mandible
Can you make the correct diagnosis?
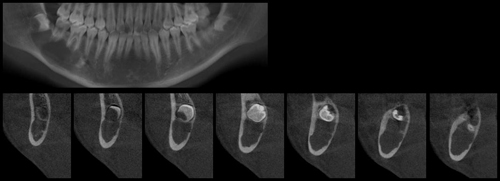
This is a 14-year-old Japanese male who presented with a large radiolucency associated with tooth #32 (Figure 1).
Sorry! you are incorrect
When examining a radiolucency that may be associated with the crown of an impacted or unerupted tooth, the clinician should first consider the possibility that it is a dentigerous cyst. Based on this radiograph, a dentigerous cyst cannot be definitively excluded. However, the presence of a scalloped radiolucency and squeezing between teeth makes a dentigerous cyst an unlikely diagnosis. The histology in this case is not supportive of a dentigerous cyst.
Dentigerous cyst is the most common developmental cyst in the oral cavity, accounting for 20% of the developmental cysts of the jaws, and is almost always associated with the crown of a tooth attached to the cemento-enamel junction as is the case in this patient. It is believed to originate from the accumulation of fluid between the reduced enamel epithelium and the tooth crown, thus expanding the follicle beyond the normal 3mm diameter (1-3). It is usually associated with impacted or un-erupted teeth. Clinically, it can be an asymptomatic radiolucency discovered during a routine dental examination or can act aggressively by expanding the jaws, leading to facial asymmetry with extreme displacement of adjacent teeth as well as the involved tooth (1-2). It can be painful and cause root resorption, especially if it is infected. It is more common in the third molars and upper canines and can also involve supernumerary teeth and odontomas. Radiographically, it presents as a smooth border, usually of unilocular or sometimes multilocular radiolucency, located around the tooth circumferentially, laterally or in the form of a “doughnut” ring. The size varies from small to extremely large, extending into the ramus of the mandible. The borders are usually corticated and smooth unless it is inflamed when loss or cortication (usually partial) is present (1). Histologically, the cyst has non-specific features lined by variable thickness of stratified squamous epithelium and supported by connective tissue. Clusters of mucous cells are frequently present, especially in the mandibular third molar areas. Treatment depends on its size, and ranges from thorough curettage to marsupialization. It usually has a good prognosis. Recurrence is uncommon if properly removed. Occasionally this cyst is associated with ameloblastoma, epithelial dysplasia and/or squamous cell carcinoma or mucoepidermoid carcinoma (1-3).
Sorry! you are incorrect
A unilocular radiolucency with a scalloped border associated with the crown of an unerupted tooth should make the clinician consider the possibility that it is an odontogenic keratocyst; this possibility may even exceed that of it being a dentigerous cyst. The radiographic findings of this case are supportive of an OKC but the histology is not.
Odontogenic keratocyst (OKC) is an aggressive odontogenic cyst and is known for its rapid growth and its tendency to invade the adjacent tissues, including bone. It has a high recurrence rate and is associated with basal cell nevus syndrome (4-5). The majority of patients are in the age ranges of 20-29 and 40-59, but cases in patients ranging in age from 5 to 80 years have been reported (4). The distribution between sexes varies from equal distribution to a male-to-female ratio of 1.6:1. OKC predominantly affects Caucasian populations and, if one may judge from the limited evidence provided by the literature, is chiefly of Northern European descent (4). Odontogenic keratocysts may occur in any part of the upper and lower jaw, with the majority (almost 70%) occurring in the mandible. They occur most commonly in the angle of the mandible extending superiorly into the ramus (4-5). Radiographically, OKCs present predominantly as unilocular radiolucencies with well-defined or sclerotic borders; they may also present as multilocular radiolucencies or, more commonly, unilocular with scalloped borders (4-5). They usually penetrate the bone rather than expand; they grow in an anterior and posterior manner with little to no expansion. The larger OKCs, however, tend to expand bone, but mildly. Obvious clinical expansion should be viewed with suspicion for a neoplasm. OKCs can also present as small and oval radiolucencies between teeth simulating a lateral periodontal cyst, in an area of an extracted tooth simulating a residual cyst, at the apex of a vital tooth mistaken for a periapical cyst, or in the anterior maxilla between the central incisors simulating an incisive canal cyst (4-5). OKCs grow to sizes larger than any other odontogenic cysts. Despite this aggressive growth, they often remain asymptomatic, thus growing to large sizes and hollowing the bone (4-5). Like dentigerous cysts, if infected, they can be painful, thus symptomatic. Multiple OKCs are frequently associated with bifid-rib basal cell nevus syndrome (Gorlin syndrome). Odontogenic keratocysts are significant clinical entities due to their tendency for recurrence and destructive behavior. They are known to have a high recurrence rate, ranging from 13% to 60% (4). Complete surgical removal is the treatment of choice. Enucleation combined with Carnoy’s solution or liquid nitrogen treatment has been effective in reducing recurrence rate (5).
Congratulations! You are correct
The jawbones are subject to many cysts, mostly of odontogenic (i.e. tooth) origin and some developmental (of both tooth and non-tooth origin), while others are cyst-like or pseudocyst structures such as the salivary gland depression and traumatic bone cavity. The traumatic bone cyst is best called a traumatic bone cavity since this condition does not represent a true cyst. Traumatic bone cavity (TBC) is not unique to the jawbones; it is also described in the long bones and is known as a simple solitary bone cyst occurring mostly in the humerus or femur, close to the epiphyseal plate (6). The long bone simple cyst is similar to the jaw traumatic bone cavity radiographically and occurs in the same age range. Trauma has been suggested as the etiology along with other non-substantiated theories such as cystic degeneration of a preexisting tumor or of the fatty marrow in the area.
Some reports suggest that it is more common in males (7) while others report equal distribution between males and females (6). The long bone counterpart is more common in males by a ratio of 2.5:1. Most reports agree that the average age of occurrence is below 20 years of age (6-7). These lesions can occur, but are uncommon, over the age of 30. Kaugars reported a higher number of TBC cases in African American females compared to the literature (6). The latter patients were over the age of 30 (6). This may suggest an association with florid cemento-osseous dysplasia. The mandible is the most commonly affected area, where over 95% of cases occur, especially in the posterior premolar-molar area. They rarely extend to the ramus; therefore this case is unique in that it extends very high into the ramus. TBCs are also known to cross the midline anteriorly. In one study, 27% of cases were anterior to the canine and some crossed the midline. They are usually unilocular and radiolucent, typically above the alveolar canal, and in many cases have a scalloped superior border spreading between the roots of teeth. The latter are vital and are frequently found hanging within the empty cavity. About 25% of the lesions occur in the anterior mandible apical to the canine tooth and are usually round and unilocular; they can therefore be mistaken for periapical lesions, leading to an unnecessary endodontic treatment. Therefore, it is important to test the vitality of the teeth and carefully examine the radiographs for changes consistent with a periapical granuloma or cyst. TBCs that are large, expansile and multilocular, as this patient’s is, have been described but are rare. Though expansion is not characteristic of TBC, it is described in about 26% of cases (6). TBCs are otherwise asymptomatic. The margins of these lesions range from very well defined to corticated to punched-out radiolucency. Pathologic fractures associated with traumatic bone cavity have been described in the jaws, but are rare. They are, however, more common in association with TBCs of the long bones.
Clinically, surgeons report an empty cavity at entrance in about two thirds of cases and straw-colored-fluid-filled cavities in about one third of cases. Blood clots are also present occasionally. The bony cavity is scraped to generate bleeding, which is considered the treatment of choice for this condition. Other methods of treatment have been tried, such as packing the curetted cavity with autogenous blood, autogenous bone and hydroxyapatite (7). Various other reports demonstrate healing of TBC after injection of autogenous blood, after aspiration and after endodontic treatment. These lesions may spontaneously heal, but rarely. Biopsy material consists of fragments of viable bone and loose connective tissue, as reported in our case. Osteoclast-like giant cells have also been described in a few cases (6). Exploration surgery usually leads to healing. Recurrence is rare.
References
- Hyomoto M, Kawakami M, Inoue M, Kirita T. Clinical conditions for eruption of maxillary canines and mandibular premolars associated with dentigerous cysts. Am J Orthod Dentofacial Orthop. 2003; 124:515-520
- Shibata Y, Asaumi J, Yanagi Y, Kawai N, Hisatomi M, Matsuzaki H, Konouchi H, Nagatsuka H, Kishi K. Radiographic examination of dentigerous cysts in the transitional dentition. Dentomaxillofac Radiol. 2004 Jan;33(1):17-20.
- Ko KS, Dover DG, Jordan RC. Bilateral dentigerous cysts–report of an unusual case and review of the literature. J Can Dent Assoc. 1999 Jan;65(1):49-51.
- Shear M. Odontogenic keratocysts: natural history and immunohistochemistry. Oral Maxillofacial Surg Clin N Am. 2003; 15: 347-362.
- Oda D, Rivera V et al. Odontogenic keratocyst: the northwestern USA experience. J Contemp Dent Pract. 2000 Feb 15; 1(2): 60-74.
- Kaugars GE, Cale AE. Traumatic bone cyst. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1987; 63: 318-324.
- Dellinger TM, Holder R et al. Alternative treatments for a traumatic bone cyst: a longitudinal case report. Quintessence Int. 1998; 29: 497-502.