Return to Case of the Month Archives
June 2009: Single small nodule lingual tooth #28
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Ken Akimoto
Bellevue, WA
Case Summary and Diagnostic Information

This is a 61-year-old white male seen at a periodontology clinic in October 2008 for an extraction and implant placement on tooth #13. Upon examination, this small (about 3mm), unilateral, exophytic, sessile and smooth-surfaced lesion was noted on the lingual gingiva of tooth #28 (Figure 1). It was of unknown duration and was asymptomatic. Radiographic findings were within normal limits with no evidence of bony involvement. The patient was unaware of its presence.
Diagnostic Information Available
This is a 61-year-old white male seen at a periodontology clinic in October 2008 for an extraction and implant placement on tooth #13. Upon examination, this small (about 3mm), unilateral, exophytic, sessile and smooth-surfaced lesion was noted on the lingual gingiva of tooth #28 (Figure 1). It was of unknown duration and was asymptomatic. Radiographic findings were within normal limits with no evidence of bony involvement. The patient was unaware of its presence.
Figure 1 Photograph taken at first clinical presentation; note the small, pink, sessile and dome-shaped and smooth-surfaced nodule on the lingual gingiva of tooth #28.
The patient’s past medical history is unremarkable.
The patient presented for the extraction of tooth #13 and was not aware of the presence of this lesion. It was small, asymptomatic, not ulcerated, and the same color as the surrounding gingiva. It was around three mm in size, exophytic and of unknown duration. It clinically resembled a small fibroma or traumatic neuroma.
Treatment
Under local anesthesia, this small nodule was completely surgically removed. The area healed without any complications.
Incisional Biopsy
Histologic examination of the H & E section revealed a small piece of soft tissue covered by keratinized epithelium and supported by dense connective tissue containing a neoplasm of odontogenic origin (Figure 2). This neoplasm occupied the bulk of the specimen and was made up of epithelial islands of variable shapes and sizes (Figure 3). These islands were lined by one layer of palisaded and polarized columnar and cuboidal epithelial cells (Figure 4). The center of the islands were filled with stellate-reticulum type epithelial cells and squamoid epithelial cells. Focal areas of cystic degeneration were also present in one or two of the neoplastic islands.
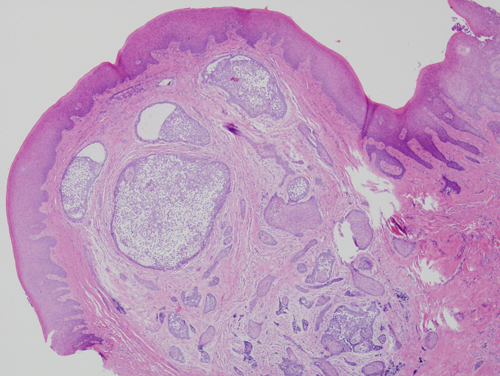
Figure 2 Low power (x40) H & E histology shows gingival covered by surface epithelium and connective tissue containing a neoplasm of odontogenic epithelial origin. This neoplasm is made up of epithelial islands of variable shapes and sizes.
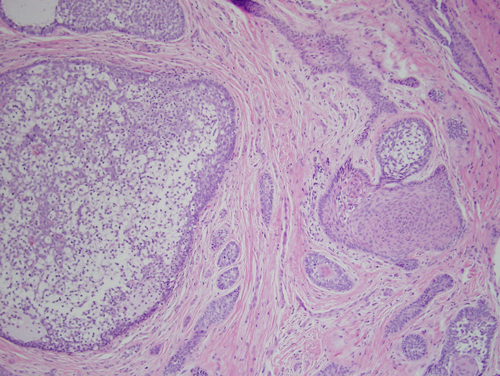
Figure 3 Higher power (x100) H & E histology taking a closer look at the epithelial islands with palisaded columnar/basaloid epithelial cells at the periphery and stellate reticulum type epithelium in the center of some of the islands and squamoid epithelium in other islands.
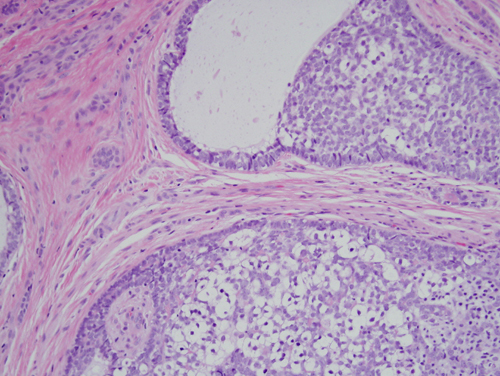
Figure 4 High power (x200) higher power H & E histology taking an even closer magnification of the epithelial islands with palisaded columnar/basaloid epithelial cells at the periphery and stellate reticulum type epithelium in the center.
After you have finished reviewing the available diagnostic information